
The Skin Disease Everyone Judges and Almost No One Understands: What's Really Driving Plaque Psoriasis
It's not dry skin, and it isn't contagious — it's a full-body immune misfire that can quietly reach the heart while it marks the skin. A rogue iron hormone.

Dermatology & Clinical Research
Plaque Psoriasis: Inside the Science of Its Causes and the Treatment Journey
What actually happens under the skin, why prevalence shifts so sharply across the map, and how new science on genes, iron, nanofibers, and biosimilars is reshaping care.
Plaque psoriasis is far more than a cosmetic skin condition. It is a chronic, immune-driven disease that alters how skin cells multiply, how immune signaling behaves, and — as newer research shows — how blood vessels and the heart function over time. Millions of people live with its raised, silvery patches and unpredictable flares, often carrying an emotional weight the skin alone doesn't explain. This piece looks at what happens beneath the surface, why prevalence differs so widely by geography, and how research into genetics, iron metabolism, nanotechnology, and biosimilar biologics is quietly changing the treatment journey.

Key Highlights
An estimated 125 million people worldwide live with psoriasis, and plaque psoriasis is its most common form.
Global prevalence sits near 0.84%, yet it ranges from under 1% in parts of Asia to above 4% in Norway and France.
A newly identified mutation in the IKBKB gene helps explain why some patients progress to psoriatic arthritis.
University of Bath scientists linked the skin hormone hepcidin to iron overload that may drive flares.
A once-daily nanofiber patch from the University of Copenhagen delivers two medicines in one dry application.
A 2026 phase 3 trial found a ustekinumab biosimilar performs equivalently through 52 weeks, widening access to biologic therapy.
Why It Matters
Plaque psoriasis is frequently dismissed as a surface-level nuisance, but the clinical record tells a different story. Roughly a third of patients also develop joint involvement, and researchers have now shown, in a mouse model, that the same chronic inflammation confined to the skin can spill over into the arteries — shortening the time it takes for a blood clot to form and inflaming vessel walls in ways that resemble early atherosclerosis. Reversing the skin disease reduced that vascular inflammation too, which is a meaningful clue that treating the skin aggressively may protect the heart.
The disease also carries a real financial weight. Health system data from Kazakhstan show that a single year's medication spending for under a thousand psoriasis patients ran into the millions of dollars, averaging in the thousands of dollars per patient — a pattern echoed across health systems that fund biologic therapy. That cost pressure is precisely why biosimilar development and delivery innovations matter: they aim to keep effective treatment within reach as demand grows.
Then there is the human side. People living with visible plaques describe being wrongly assumed to have poor hygiene, and researchers studying the disease's genetics note that stigma remains one of its most under-addressed burdens. Understanding the biology isn't just academic — it is the groundwork for treatments that are cheaper, gentler to use, and easier to stay consistent with.
Detailed Viewpoint
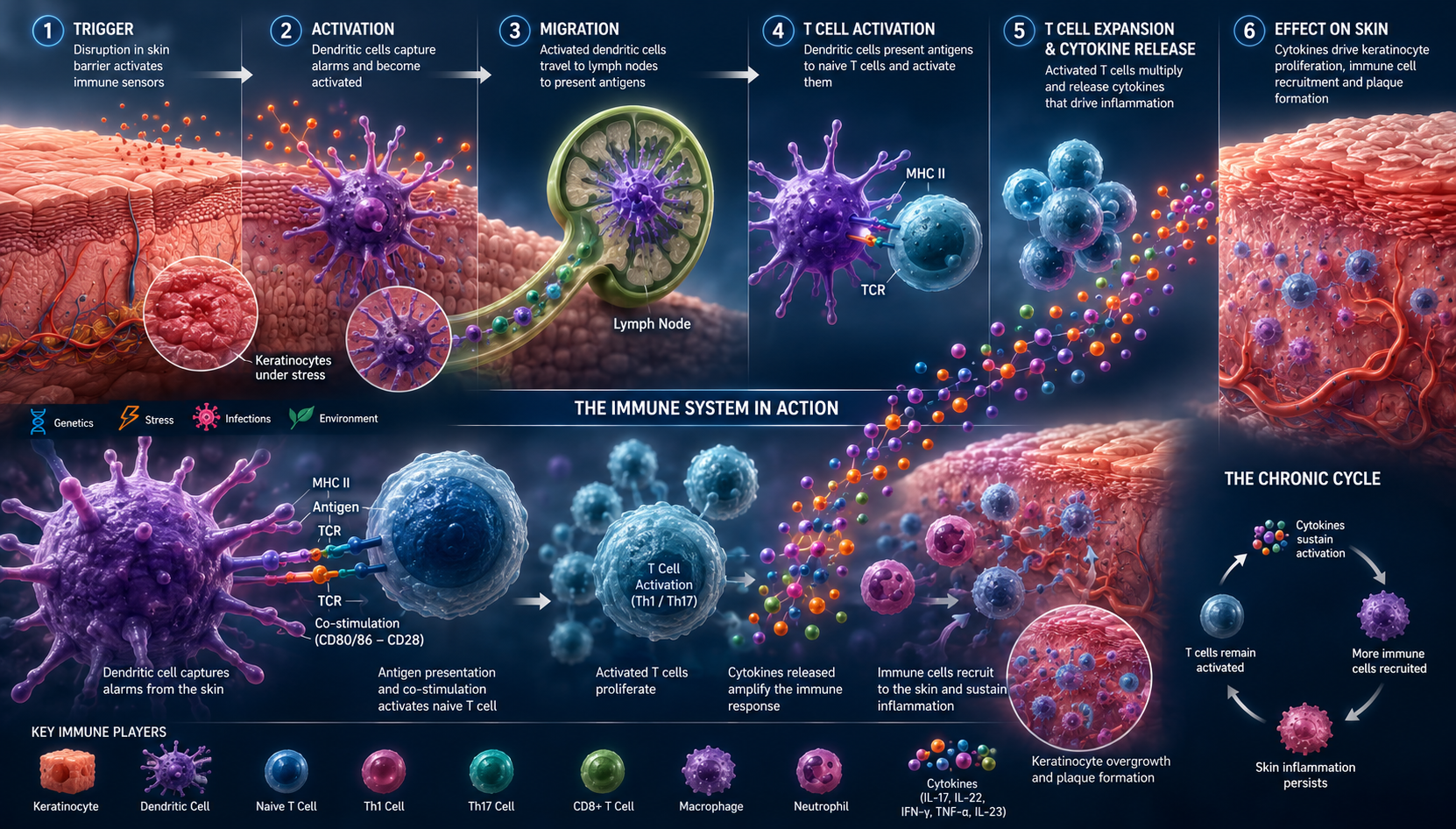
What Happens Inside the Skin
Plaque psoriasis is a chronic, non-infectious disease driven by an overactive immune response rather than a skin infection or poor hygiene. Immune signaling pushes skin cells to multiply far faster than normal, and the excess cells pile up on the surface as raised, well-demarcated plaques covered in silvery-white scale, most often on the elbows, knees, scalp, and lower back. Even minor skin trauma — a scratch, a friction point, a cut — can trigger a new plaque to form along that exact line, a pattern dermatologists call the Koebner response. The course is unpredictable: some people cycle through remission and flare for decades, and factors like stress, alcohol, smoking, and family history tend to predict a rougher path.
A Disease That Changes by Map
A 2024 literature review covering global and regional data found that plaque psoriasis prevalence is anything but uniform. Rates run highest in colder, higher-income regions of Western Europe and North America — Norway near 4.6%, France near 4.4%, Portugal near 4.4%, and the United States around 3% — while parts of Asia and the Asia-Pacific region report figures under 1%, a gap researchers partly attribute to underdiagnosis rather than true absence of disease. Kazakhstan's own reported prevalence has varied widely, from under 1% to roughly 2.5%, depending on the study and region. Onset tends to follow a bimodal pattern, clustering around ages 30–40 and again near 60, and the disease affects men and women in roughly comparable numbers, though the split shifts slightly from country to country.
Two Fresh Clues to the Root Cause
Two 2024 discoveries reframe how researchers think about what actually starts the disease. At the Australian National University, scientists identified a mutation in the IKBKB gene that disrupts regulatory T cells — the immune system's normal peacekeepers — causing them to fuel inflammation instead of containing it. Patients carrying two copies of the mutated gene appear more likely to progress from skin-only psoriasis to psoriatic arthritis, offering a possible explanation for why joint disease develops in some people and not others. Separately, a University of Bath–led team found that the iron-regulating hormone hepcidin, normally produced only in the liver, is also generated directly in psoriatic skin. That local hepcidin appears to trap excess iron in skin cells, triggering both runaway cell growth and a build-up of inflammatory neutrophils — the two hallmarks of a plaque. The finding is especially relevant for pustular psoriasis, a severe and often treatment-resistant subtype, and points toward hepcidin-blocking drugs as a genuinely new category of therapy rather than another variation on existing immune-pathway blockers.
Rethinking How Treatment Reaches the Skin
Delivery, not just the drug itself, is a major barrier to consistent treatment. Creams and ointments typically need to be applied multiple times a day, feel greasy, and are frequently abandoned partway through a course — researchers estimate that around a third of patients never receive treatment at all, in part because the regimens themselves are hard to sustain. In response, University of Copenhagen researchers built a dry, electrospun nanofiber patch that holds two active ingredients and releases them at different speeds: salicylic acid immediately, to lift dead surface cells, and hydrocortisone more gradually, to calm inflammation over time. Early testing on pig skin and human skin cells found the patch performed comparably to standard creams while requiring only one application a day, and the same underlying platform may eventually extend to eczema and wound care. A separate nanotechnology study out of the University of Macau examined how particle size affects the way immune dendritic cells and the skin's lymphatic system absorb and transport psoriasis drugs, offering a design principle — bigger carriers favor local skin uptake, smaller ones travel further into lymph nodes — that could inform how future topical and injectable psoriasis therapies are engineered.
From Topical Creams to Biologics — and Now Biosimilars
Standard care still follows a stepwise ladder: topical corticosteroids and vitamin D analogues for mild disease, phototherapy for moderate cases, and systemic drugs or biologic injections for moderate-to-severe disease that doesn't respond to milder options. Newer non-steroidal topicals are widening the first rung of that ladder — a pooled review of phase III trials for the topical PDE4 inhibitor roflumilast found that 37–42% of patients reached clear or almost-clear skin at eight weeks, compared with roughly 6–7% on the inactive control cream, with similar success sustained to week 52. Further up the ladder, biologic drugs that block IL-12/IL-23 signaling, such as ustekinumab, have become a mainstay for moderate-to-severe disease, though their cost has long limited access. That is starting to shift: a randomized phase 3 trial completed in 2026 compared a ustekinumab biosimilar against the original biologic in more than 500 patients and found closely matching skin-clearance rates, safety profiles, and antibody responses through a full year of treatment, including in patients who switched from the reference drug partway through. Results like these are part of why regulators in the United States have approved ustekinumab biosimilars for the market — a shift that, over time, should make biologic-level psoriasis control more affordable for more patients.
The Road Ahead
There is still no cure, and every treatment on the ladder carries trade-offs — skin thinning from long-term steroids, infection risk from immune-suppressing biologics, and the practical burden of frequent applications or injections. But the direction of the last two years is encouraging: researchers are no longer only refining existing immune-pathway blockers, they are identifying entirely new triggers like hepcidin and IKBKB, engineering delivery systems that ask less of the patient, and building a biosimilar pipeline that could finally close the affordability gap. For a disease this common and this often underestimated, that combination — new science plus wider access — is what a real treatment journey looks like.

Citation & Credibility
This article draws on peer-reviewed research, university press releases, and clinical publications. Sources include the StatPearls (NCBI Bookshelf) clinical reference on plaque psoriasis; a 2024 epidemiology and economic-burden review in the Journal of Clinical Medicine of Kazakhstan; a 2026 phase 3 biosimilar clinical trial; and research news from the University of Copenhagen, University of Bath, Australian National University, University of Macau, and Case Western Reserve University School of Medicine, along with a topical roflumilast review from the University of Southern Denmark. Figures on prevalence, incidence, and economic burden are approximate and reflect the ranges reported across the cited studies rather than a single universal statistic.
Tags
Editorial Note
This article is intended for general educational purposes and reflects publicly available research current as of mid-2026. It is not a substitute for personalized medical advice — anyone managing plaque psoriasis, or concerned about symptoms consistent with it, should consult a dermatologist or qualified healthcare provider for diagnosis, treatment planning, and monitoring.
Written by
MedBary Team
Comments
Log in to join the conversation.
Loading comments…