
The Hidden ADHD: Why Girls and Women Are Still Slipping Through the Cracks
Girls are taught to hold it together. Women are taught to push through. But behind that composed exterior, ADHD is reshaping lives in silence — and the medical system is only beginning to catch up.

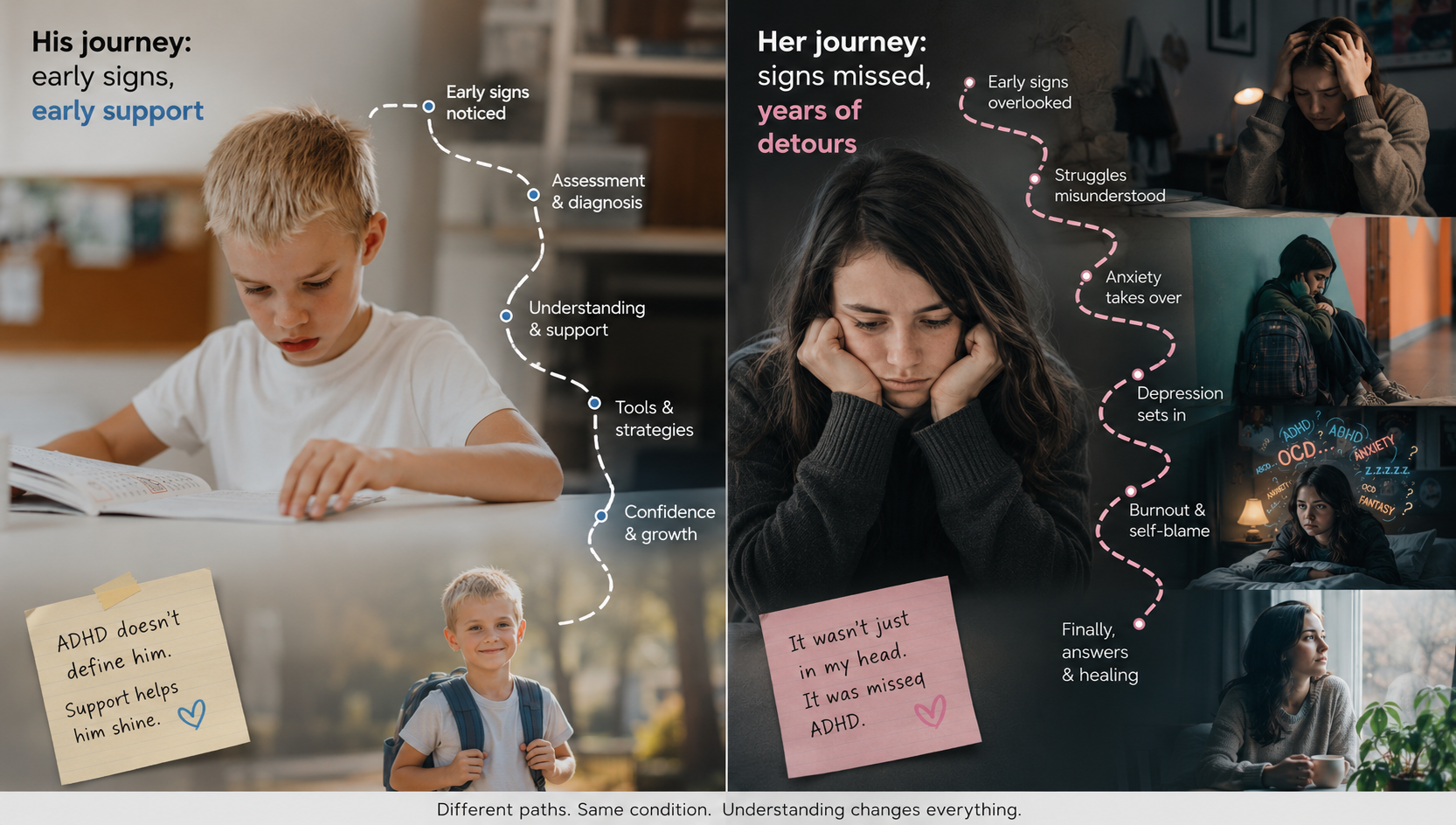
ADHD is one of the most heritable neurological conditions in medicine, yet diagnostic frameworks were built almost entirely on studies of boys. When clinicians learned to spot ADHD, they learned to look for impulsivity, physical restlessness, and classroom disruption — traits that appear far more often in males. The result is a diagnostic blind spot that has left millions of women without answers during the years they needed them most.
Research published in European Psychiatry examined 900 adults with confirmed ADHD diagnoses and found that women experienced significantly higher rates of depression and anxiety, reported greater daily functional impairment, and — despite symptoms beginning at the same age — received their diagnosis years later. These are not marginal differences. They reflect a systemic pattern that clinicians, educators, and families urgently need to understand.
Every year that a woman goes undiagnosed is a year she is more likely to develop secondary depression, more likely to blame herself for her struggles, and less likely to access accommodations in school or the workplace. The stakes are high enough that getting this right is not merely a matter of clinical accuracy — it is a matter of equity.

Social conditioning plays a direct role in why ADHD is underdetected in girls. From an early age, girls receive stronger cultural pressure to sit still, be agreeable, and manage their emotions without outward disruption. A girl who loses focus in class learns quickly that daydreaming is safer than fidgeting. A girl who feels overwhelmed finds that perfectionism provides a socially acceptable shell. Over time, these coping strategies become so ingrained that neither the girl herself nor the adults around her recognize the effort required to maintain them.
Clinicians describe this as masking — the active suppression or compensation of ADHD symptoms to meet social expectations. A 2024 study from Health and Care Research Wales confirmed that later diagnosis in girls is linked to this masking behavior, and that the psychological cost of sustained masking includes elevated rates of burnout, identity confusion, and emotional exhaustion.
The interplay between ADHD and female hormones remains frustratingly underfunded as a research area. Estrogen influences dopamine transmission — the very neurological pathway most disrupted by ADHD. This means that as estrogen fluctuates across the menstrual cycle, through pregnancy, postpartum recovery, and menopause, ADHD symptoms often intensify in ways that have no parallel in male physiology.
Many women report that their most severe periods of ADHD dysfunction coincide with hormonal transitions that were never connected to attention regulation. Postpartum cognitive difficulties, perimenopausal brain fog, and premenstrual attention crashes are frequently attributed to hormone changes alone — when in reality, they may represent ADHD symptoms unmasked by hormonal shifts.
Standard ADHD assessments rely heavily on behavioral rating scales completed by parents and teachers. These tools capture what adults observe — and what is observable differs profoundly by gender. A boy who shouts out answers and cannot stay in his seat registers concern. A girl who stares out the window while keeping her desk immaculate does not. The rating scale returns "no concerns" not because she has no concerns, but because her concerns are invisible to the rater.
Duke University's psychiatry faculty have noted that girls with ADHD are more likely to present with inattentive-type symptoms — difficulty sustaining focus, losing items, becoming mentally exhausted by routine tasks — rather than the hyperactive-impulsive profile that rating scales were originally designed to flag. Researchers have advocated for sex-sensitive diagnostic instruments since the 1990s. Progress has been slow.
For many women, ADHD does not become visible until adult life stacks enough demands that masking simply stops working. A new job, a first child, a relationship breakdown, a move — any single transition can overwhelm a compensatory system that was never built to handle real volume.
Women diagnosed in their 30s, 40s, and beyond commonly describe receiving a diagnosis not as shocking, but as profoundly clarifying — and then profoundly painful. The relief of finally having an explanation is real. So is the grief for the years spent fighting a hidden battle with no name and no support. Diagnosis in adulthood is better than no diagnosis. But it is not equivalent to early identification, and the field cannot continue treating late diagnosis as an acceptable outcome.
| Presentation Area | Boys / Men | Girls / Women |
|---|---|---|
| Primary symptom type | Hyperactive, impulsive, externalized | Inattentive, internalized, emotional |
| Classroom behavior | Disruptive, visible to teachers | Quiet, overlooked, "daydreamer" |
| Coping mechanisms | Acting out, higher substance use rates | Perfectionism, people-pleasing, masking, substance use rates |
| Co-occurring conditions | Conduct disorder, substance use | Anxiety, depression, eating disorders, substance use |
| Average age at diagnosis | Earlier — often childhood | Later — adolescence or adulthood |
Written by
MedBary Team
Comments
Log in to join the conversation.
Loading comments…