
Beyond the Waiting List: 3D Bioprinting and the Future of Kidney Transplantation
Every 18 minutes, someone joins a kidney transplant list with nowhere to turn. 3D bioprinting may finally change that math.

Every eighteen minutes, a new patient is added to a kidney transplant waiting list somewhere in the world — yet the supply of donor organs has barely moved in decades. Now, a convergence of stem cell biology, advanced biomaterials, and precision 3D bioprinting is threatening to make organ scarcity a solvable engineering problem rather than an immovable humanitarian tragedy. This article examines where the science stands, what the obstacles remain, and why the next decade may be the most consequential period in transplant medicine since the first successful kidney transplant in 1954.

Why It Matters
850M
people worldwide live with some form of kidney disease
37M
Americans affected — dialysis or transplant are the only current options
5,000+
patients die on the US waiting list every single year
The scale of kidney failure is staggering, and it is quietly worsening. Diabetes and hypertension, both rising globally, are the two leading causes of end-stage renal disease. When kidneys fail entirely, dialysis extends life but extracts an enormous toll: patients endure treatment sessions several times per week, face persistent risks of infection and vascular complications, and report dramatically reduced quality of life. No meaningfully new clinical solution has emerged since the 1960s.
Transplantation remains the gold standard — it extends life, restores function, and dramatically improves wellbeing, but the organ supply cannot scale with demand. The mathematics are unforgiving: five people die for every transplant that happens in the United States. Bioprinting matters because it is the first technology with a credible pathway to manufacturing kidneys on demand, at scale, using a patient's own cells — eliminating both the donor bottleneck and the lifelong immunosuppression burden simultaneously.
Beyond transplantation, 3D-printed kidney tissue already functions today as a superior drug-testing platform. Kidney organoids — miniature, functionally accurate kidney models — allow pharmaceutical researchers to screen drug toxicity far more accurately than animal models, potentially preventing the kind of late-stage clinical trial failures that cost billions and delay treatments by years.

Detailed Viewpoint
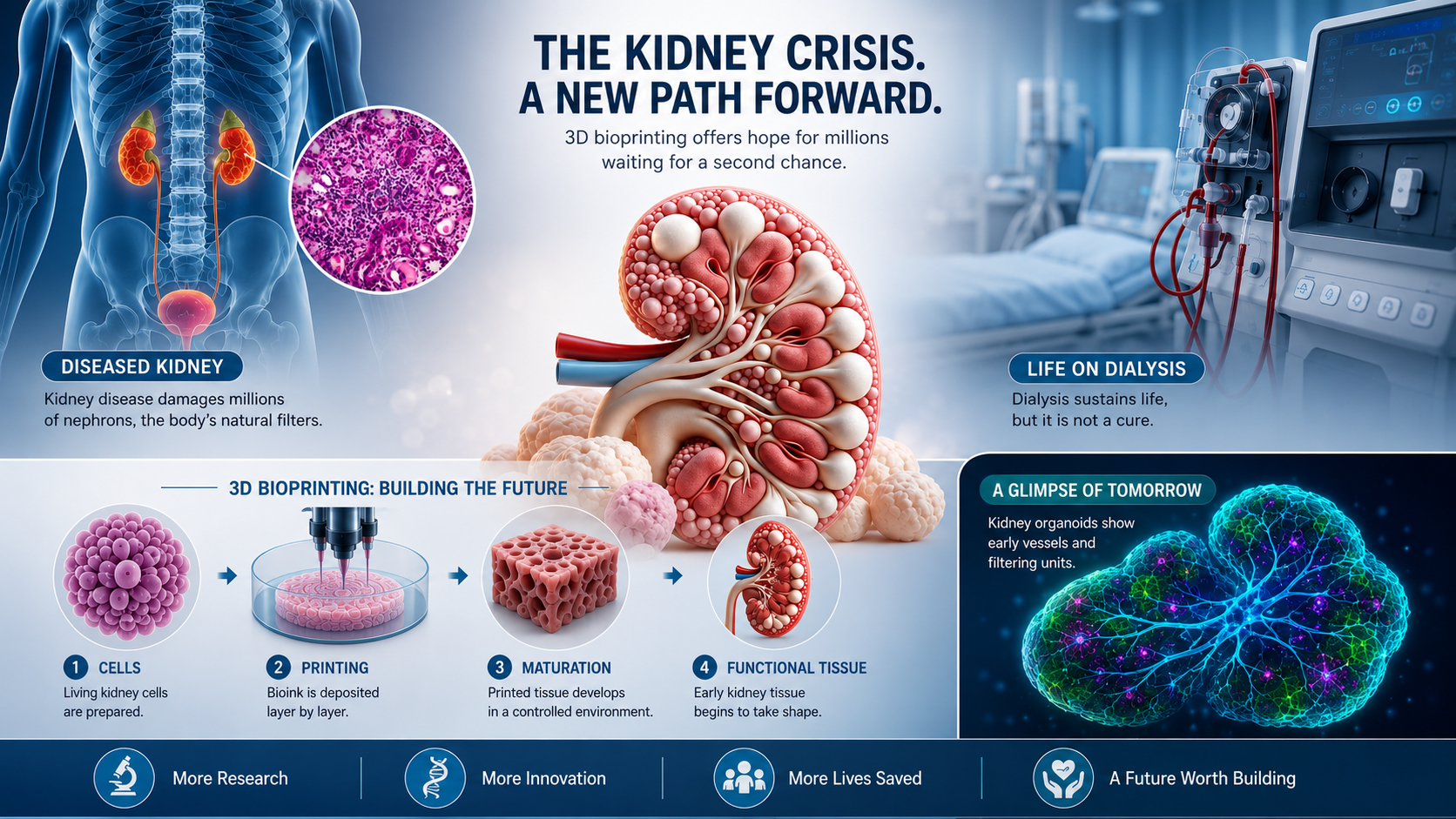
How 3D Bioprinting Actually Works
Unlike conventional 3D printing, which works with plastics or metals, bioprinting uses "bioinks" — living cells embedded within supportive hydrogel scaffolds — as its raw material. These inks are loaded into specialized printheads and deposited with micron-scale precision, building tissue architecture layer by layer according to a digital blueprint derived from medical imaging. The scaffolding material degrades over time as the cells mature and establish their own extracellular matrix, ideally leaving behind functional tissue that behaves like the real thing.
For kidneys specifically, the challenge is extraordinary. The human kidney contains roughly one million nephrons — the functional filtration units — each comprising multiple distinct cell types arranged in precise spatial relationships. Recreating this complexity at scale, while simultaneously embedding a vascular network capable of supplying oxygen and nutrients deep within thick tissue, has been the field's central engineering problem for two decades.
The SWIFT Breakthrough at Harvard's Wyss Institute
"A swifter way towards 3D printed organs" — the SWIFT technique dissolves temporary sacrificial channels inside living tissue, leaving behind a web of hollow passages that become the organ's blood vessel network.
Researchers at Harvard's Wyss Institute addressed the vascularization problem through a technique called Sacrificial Writing in Functional Tissue (SWIFT). The method embeds a temporary, sacrificial material within a living cellular matrix and later dissolves it away, leaving behind a network of hollow channels that can be perfused with blood-like fluids. This breakthrough, developed in the lab of Jennifer Lewis, Sc.D., cracked open the possibility of fabricating thick, viable kidney tissue that would not simply die at its core from lack of oxygen.
Complementing this, collaboration with clinical researchers — including Joseph Bonventre, M.D., Ph.D., of Brigham and Women's Hospital — enabled the team to generate kidney organoids from human stem cells and then culture them under conditions of fluid flow. This mimics the mechanical environment of a real kidney, prompting the organoid cells to mature and establish more physiologically accurate vascular networks. These advances were subsequently licensed to Trestle Biotherapeutics, which is advancing them toward clinical application.
The Stem Cell Advantage: Solving Rejection
Immune rejection is the Achilles' heel of conventional transplantation. Even with the best immunological matching and modern immunosuppressant drugs, the recipient's immune system recognizes a donor kidney as foreign and mounts an attack over time — eventually failing half of all transplanted kidneys within ten to fifteen years. Patients must take powerful drugs for life, drugs that carry their own burden of infections, cardiovascular side effects, and increased cancer risk.
Bioprinting with induced pluripotent stem cells (iPSCs) derived from the patient themselves fundamentally rewrites this equation. Because the bioink cells carry the patient's own genetic signature, the printed tissue is immunologically self — the body should recognize it as belonging, not foreign. If this holds in clinical practice, it would eliminate the need for lifelong immunosuppression and transform the risk profile of kidney replacement therapy entirely.
From Patient to Printed Organ: The Core Workflow
| Stage | Process | Current Status |
|---|---|---|
| 1. Cell Sourcing | Skin or blood cells from patient reprogrammed into iPSCs | ✓ Established |
| 2. Differentiation | iPSCs guided to become kidney-specific cell types | ✓ Advanced |
| 3. Bioink Formulation | Cells embedded in hydrogel scaffold material | ⟳ Active R&D |
| 4. Bioprinting | Layer-by-layer deposition with vascular channel formation | ⟳ Pre-clinical |
| 5. Maturation | Bioreactor conditioning to develop structure and function | ⟳ Active R&D |
| 6. Implantation | Surgical placement as functional kidney replacement | ◷ Future Goal |
The Current Frontier: What Has Been Achieved
Research teams globally have now demonstrated functional kidney organoids — miniaturized, self-organized structures that replicate many core features of kidney biology. These are not yet transplantable kidneys, but they filter waste, respond to drugs, and even develop early disease states in response to toxins, making them invaluable as research and screening tools.
The field of bioprinting itself has recognized this category of work as historically significant. PMI included 3D kidney bioprinting among its 2024 Most Influential Projects — a list that acknowledges not just technical achievement but transformative real-world potential. Meanwhile, Australia's Royal Society of Victoria published reporting in early 2025 documenting the field's transition from laboratory curiosity to systematic clinical research agenda, with dozens of groups worldwide now publishing results on vascularized renal organoids and hybrid bioprinting approaches.
The Obstacles That Remain
Despite genuine and accelerating progress, the path from today's organoids to tomorrow's implantable kidneys is still measured in years of research and billions of dollars of investment. Several challenges stand between the current state of the art and clinical reality:
Vascularization at scale. Embedding a complete, functional capillary network throughout a full-sized organ — with vessels down to 10 micrometres in diameter — remains at the frontier of what current printing resolution can achieve.
Cell maturity. Stem-cell-derived kidney cells in organoids often resemble fetal kidney tissue rather than fully adult cells. Ensuring the printed organ achieves full adult function before implantation is an active and unsolved challenge.
Regulatory pathways. Living, patient-specific organs occupy a category that existing medical device and tissue regulatory frameworks were not designed for. New evaluation frameworks are needed before any bioprinted organ can reach first-in-human trials.
Manufacturing cost and time. The process of collecting patient cells, reprogramming them, differentiating them, formulating bioinks, printing, and maturing tissue currently takes weeks to months and remains expensive. For this to reach patients at meaningful scale, the economics need to change significantly.
Despite these barriers, the directionality of the research is unmistakably forward. Each published study narrows the gap between proof-of-concept and clinical reality. The field's most serious scientists speak not of whether transplantable bioprinted kidneys will arrive, but when — and most estimates, cautiously, place first human implantation within the 2030s.
Citations & Credibility
This article draws on peer-reviewed research, institutional publications, and recognized science journalism. All factual claims about organ shortage statistics, technology capabilities, and clinical status are grounded in the sources listed below.
Wyss Institute at Harvard University
Kidney Engineering Technology for New Tissue Replacement Therapies. Jennifer Lewis, Sc.D., and Joseph Bonventre, M.D., Ph.D. Published 2021, updated 2023.
wyss.harvard.edu/technology/kidney-engineering-technology…PubMed Central / NIH — PMC10607284
Peer-reviewed research on 3D bioprinting of renal tissues and kidney organoids. National Institutes of Health — National Library of Medicine.
pmc.ncbi.nlm.nih.gov/articles/PMC10607284/Project Management Institute (PMI)
2024 Most Influential Projects — 3D Kidney Printing. PMI recognition of global significance in biomedical engineering.
pmi.org/most-influential-projects-2024/3d-kidney-printingRoyal Society of Victoria — Science Victoria Magazine
"From Ink to Organ: The Power of 3D Bioprinting." Haireya Abudureheman, University of Melbourne. Jan–Feb 2025 Biotechnology Edition.
rsv.org.au/articles/bioprintingStatistical data on US transplant waiting lists and annual deaths sourced from the Wyss Institute publication, which cites UNOS/OPTN registry data. Global disease burden figures (850 million) per the Wyss Institute report citing National Kidney Foundation epidemiology. Australian waiting list figures per RSV Science Victoria reporting.
Article Tags
Editorial Note
This article is intended for general medical and science literacy purposes and does not constitute clinical or medical advice. The field of 3D bioprinting is rapidly evolving; readers seeking the most current clinical data are encouraged to consult peer-reviewed publications and institutional research portals directly. Statistics cited reflect figures available from referenced sources and may have been updated since publication.
Written by
MedBary Team
Comments
Log in to join the conversation.
Loading comments…