There Aren't Enough Hearts to Go Around. So Engineers Built One.
There are 23 million patients. There are 6,000 donor hearts. The gap is where the engineering begins.

Heart failure is not a disease of the elderly. It strikes people in their thirties and forties — accelerated by viral myocarditis, inherited cardiomyopathy, and complications from other chronic conditions. More than 23 million people worldwide live with some degree of heart failure, and a significant fraction progress to a stage where medication, stents, and conventional surgery can no longer sustain the organ.
A transplant remains the cleanest solution — but donor organ supply is structurally incapable of meeting demand. Roughly 6,000 donor hearts become available globally each year, a figure that has stayed largely flat for two decades despite expanded awareness campaigns. The mathematics of that gap is unforgiving.
Mechanical circulatory support — from partial-assist pumps working alongside a still-beating heart to devices that replace the failing ventricles entirely — represents the only scalable alternative. A durable, implantable total artificial heart could fundamentally reorder the global transplant system: easing organ waiting lists and opening treatment pathways for patients currently ineligible for transplant due to body size, age, or secondary conditions.

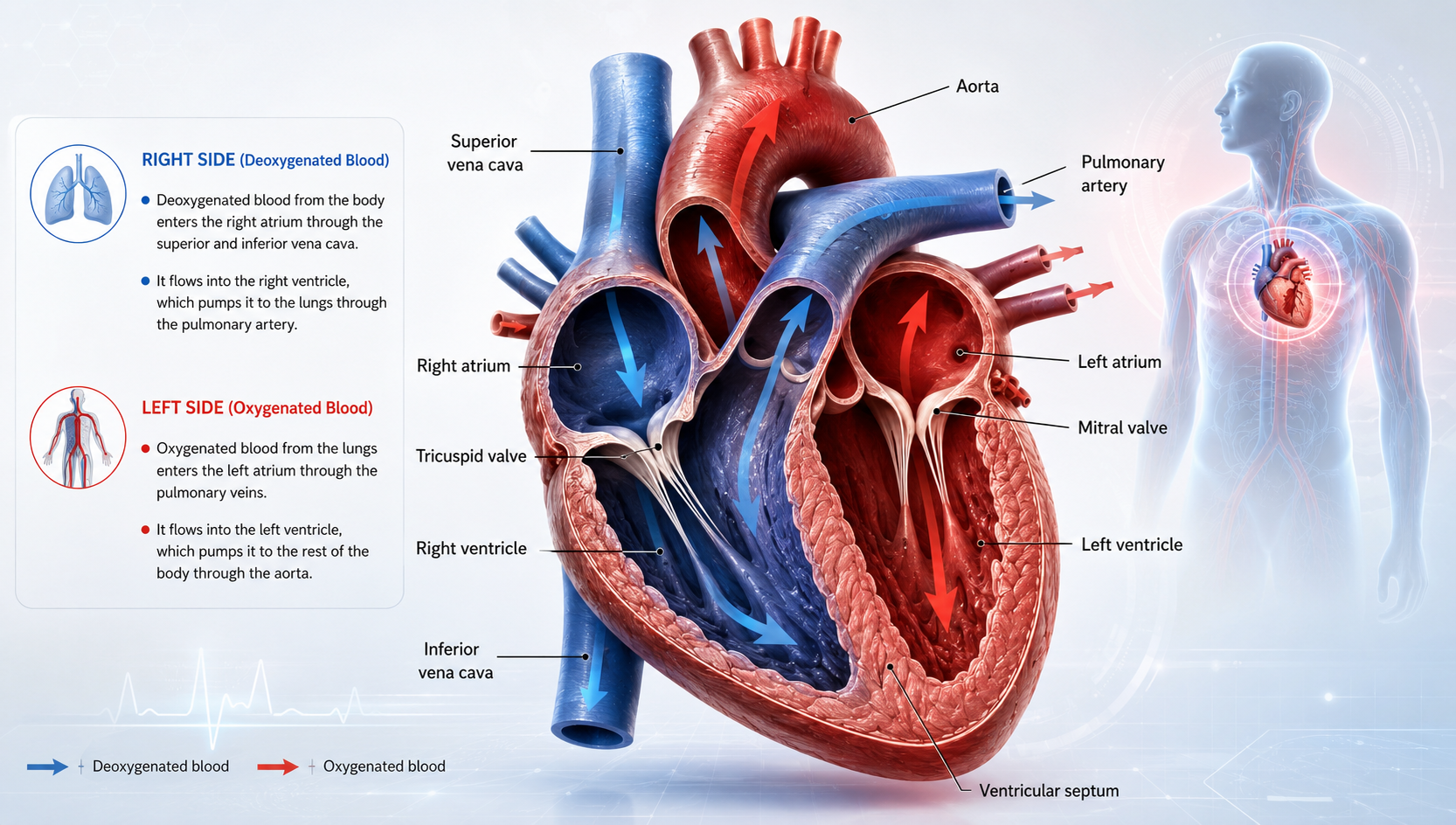
The human heart is two separate pumps sharing one housing. The right side draws oxygen-depleted blood from the body and routes it to the lungs. The stronger left side receives oxygenated blood returning from the lungs and drives it through the aorta to every organ — roughly 100,000 times a day, without conscious effort.
Advanced heart failure collapses this efficiency. Around 85 to 90 percent of end-stage patients experience left-side failure first — the left ventricle weakens progressively until it can no longer maintain adequate pressure. For this majority, a Left Ventricular Assist Device (LVAD) is the appropriate intervention: a pump implanted alongside the still-present natural heart, drawing blood from the left ventricle and injecting it into the aorta. It can generate up to 10 litres per minute, compensating for what the failing ventricle can no longer deliver — while the patient's own heart continues contributing whatever function it retains.
For the remaining ten to fifteen percent of end-stage cases, both ventricles deteriorate simultaneously. Biventricular failure places patients beyond what any LVAD can address — and it is here that a Total Artificial Heart becomes the only mechanical option. The procedure involves surgically removing both failing ventricles and all four native heart valves, then implanting a device that assumes complete circulatory function: pumping blood to both the lungs and the body independently.
"The BiVACOR Total Artificial Heart ushers in a whole new ball game for heart transplant both in Australia and internationally. Within the next decade we will see the artificial heart becoming the alternative for patients who are unable to wait for a donor heart or when a donor heart is simply not available."
Prof. Chris Hayward — Victor Chang Cardiac Research Institute & St Vincent's Hospital Sydney
Prior artificial hearts — including the Jarvik 7, which kept its first recipient alive for 112 days after implantation in December 1982 — relied on pulsatile mechanical action mimicking the natural heartbeat. This introduced substantial wear and limited device longevity. The BiVACOR Total Artificial Heart, developed by Queensland-born engineer Daniel Timms, abandons that logic entirely. It uses a single rotating titanium disc suspended within a magnetic field: no physical bearings, no direct mechanical contact. Blood is directed to both the pulmonary and systemic circuits by varying the speed and tilt of that single component — fewer moving parts, fewer failure points.
The device is compact enough for paediatric patients — a major departure from earlier designs that excluded smaller adults and children by size. Its target operational lifespan exceeds ten years. Engineers are working toward a fully implantable version where external battery connections are replaced by transcutaneous electromagnetic charging — the same principle as a wireless phone charger, delivering power across intact skin.
The world's first BiVACOR implant took place on 9 July 2024 at the Texas Heart Institute in Houston — a 58-year-old man with end-stage biventricular failure. Four further procedures followed in the United States. On 22 November 2024, Dr Paul Jansz led a six-hour surgery at St Vincent's Hospital Sydney — the sixth BiVACOR implant globally and the first outside the United States.
That patient was discharged in early February 2025 — the first person in the world to leave a clinical facility carrying a BiVACOR device. He subsequently received a donor heart transplant on 6 March 2025, after 105 days supported by the artificial heart — the longest BiVACOR bridge-to-transplant period on record.
This sits within the Monash University-led Artificial Heart Frontiers Program — backed by a $50 million grant from Australia's Medical Research Future Fund — developing three distinct mechanical circulatory support devices simultaneously. By 2036, the program projects a $1.8 billion benefit to the Australian economy and more than 2,000 new jobs in a domestic cardiac device industry that does not yet exist at scale.
Day-to-day life involves real practical adjustments. Power arrives via external batteries connected through a driveline — an electrical cable exiting the body through a small skin opening. Batteries require regular recharging; patients carry backups. The driveline exit point is the primary infection risk, a vulnerability engineers are working to eliminate through fully subcutaneous power delivery in the next generation.
Contact with water requires purpose-designed waterproof coverings. The rotating disc produces a continuous low-level sound most patients adapt to within weeks. Blood-clot risk is managed with anticoagulation therapy — which simultaneously elevates the risk of bleeding events. Research has documented that mechanical assist devices alter blood-component behaviour and affect vascular repair, a side-effect under active investigation. The tradeoff remains strongly in the device's favour for patients who would otherwise not survive to transplant.
In parallel with mechanical device development, researchers at the University of Toronto have demonstrated that immune-cell-derived nanoparticles can stimulate blood vessel formation in lab-grown human cardiac tissue — a foundational step toward constructing living, functional heart muscle in the laboratory. While fully bioengineered hearts remain years from clinical use, this research converges with mechanical programmes toward the same goal: freeing patients from dependence on donor organ availability entirely. The artificial heart of 2025 is a bridge. The question researchers are now seriously asking is whether it needs to remain one.

This article draws on publicly available institutional research, clinical announcements, and peer-reviewed publications as of mid-2025. Economic projections are sourced from Monash University's official programme documentation. Clinical timelines and procedural details reflect those reported by St Vincent's Hospital Sydney and the Victor Chang Cardiac Research Institute.
This piece is intended to inform general readers and does not constitute clinical guidance. Individuals with heart failure should consult a qualified cardiologist or specialist heart failure team about treatment options appropriate to their circumstances.
Written by
MedBary Team
Comments
Log in to join the conversation.
Loading comments…