Sleep & Obesity: The Vicious Cycle
How poor sleep drives weight gain and how excess weight destroys your sleep. Inside the bidirectional biology that most weight-loss advice ignores.

Every night you skimp on sleep, your body quietly tips the hormonal scales toward hunger, fat storage, and fatigue — making the next night's rest even harder to get. Sleep deprivation and obesity do not simply co-exist; they amplify each other in a self-reinforcing loop that most conventional weight-loss advice never addresses.
This article unpacks the bidirectional biology linking insufficient sleep to weight gain, examines the hormonal and metabolic mechanisms at work, and explains why breaking this cycle demands as much attention to the bedroom as to the kitchen.

Obesity and inadequate sleep have both reached epidemic proportions across industrialised nations. Yet most weight-loss programmes focus almost entirely on diet and exercise, largely ignoring sleep — even though the hormonal disruption triggered by sleep loss can directly undermine the dietary restraint those programmes depend on.
The consequences extend well beyond waistlines. Chronic sleep loss is independently associated with elevated cardiovascular risk, impaired glucose metabolism, and weakened immune function. When compounded by obesity, those risks multiply: obstructive sleep apnea (OSA) — a condition that obesity both causes and worsens — has been linked to stroke, heart failure, type 2 diabetes, and premature death.
"Sleep disorders and obesity are so common, and so frequently found together, that treating one without addressing the other is likely to produce limited results."
— Adapted from clinical commentary, UT Southwestern Medical Center, 2022
Financially, the burden is staggering. The global cost of obesity-related illness — spanning sleep disorder management, cardiovascular care, and diabetes treatment — already runs into hundreds of billions of dollars annually. A clearer understanding of the sleep-obesity nexus opens a direct pathway to more effective, integrated prevention.

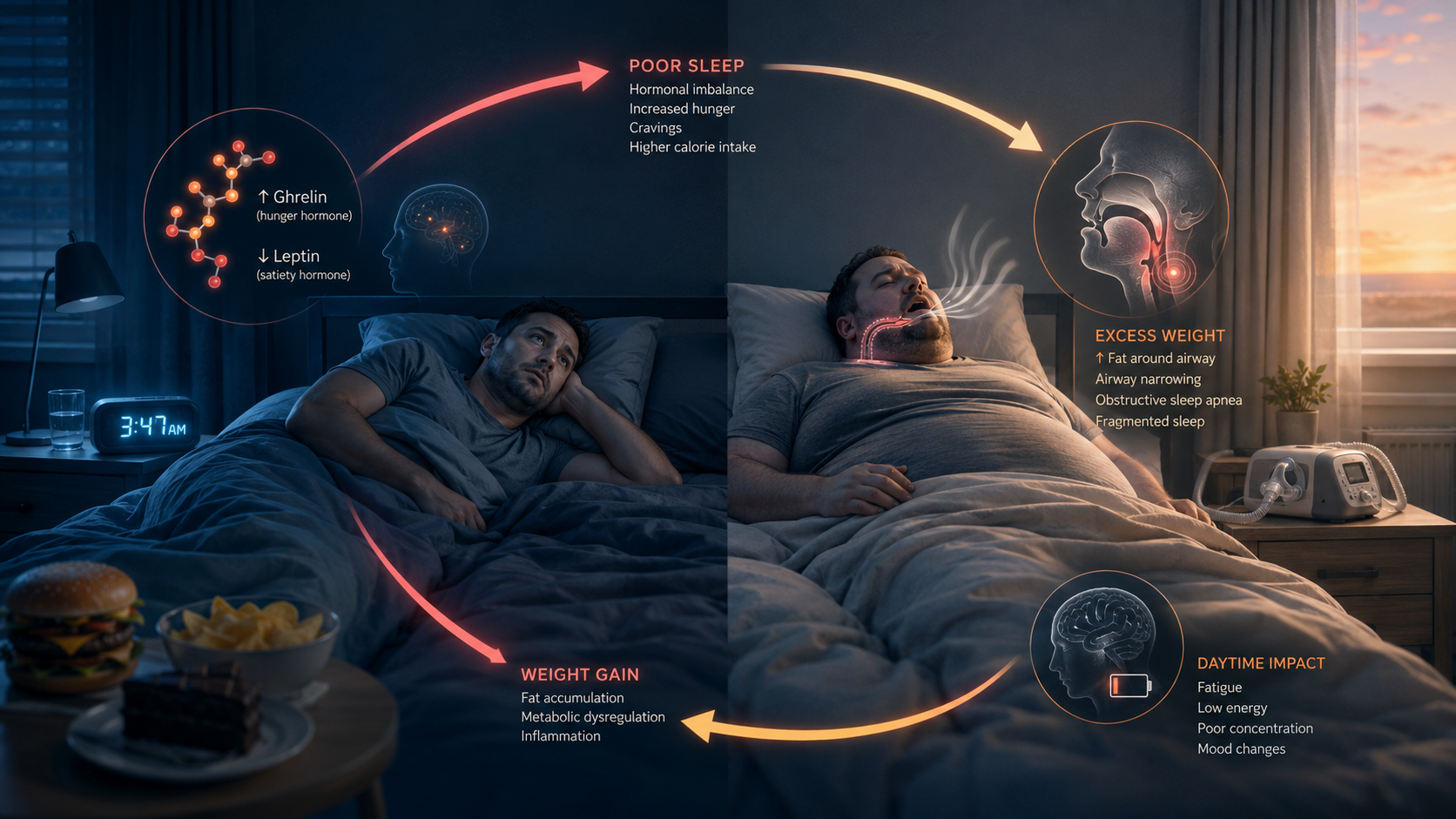
When sleep is cut short, the body interprets the deficit as a low-level physiological threat and triggers a hormonal cascade poorly suited to modern sedentary life. Two appetite-regulating hormones sit at the centre of this cascade: ghrelin and leptin.
Ghrelin — the hunger-stimulating hormone produced primarily in the stomach — rises significantly when sleep is shortened, signalling the brain to seek food even when caloric requirements have been met. Leptin, the satiety hormone produced in fat cells, works in the opposite direction: inadequate sleep suppresses its levels, blunting the feedback signal that ordinarily tells the brain the body is full. The combined effect is a powerful double-push toward overconsumption — more hunger signalling and less satiety signalling simultaneously.
| Hormone | Normal role | Effect of sleep loss |
|---|---|---|
| Ghrelin | Signals hunger; rises before meals | ↑ Increases — drives appetite upward |
| Leptin | Signals satiety; suppresses hunger | ↓ Decreases — satiety signals blunted |
| Cortisol | Stress hormone; mobilises energy reserves | ↑ Elevated — promotes fat storage and wakefulness |
| Insulin | Regulates blood glucose absorption | ↑ Resistance rises — elevates diabetes risk |
Cortisol — the quintessential stress hormone — elevates during disrupted sleep, flooding the bloodstream with glucose while simultaneously directing the body to retain, not burn, energy stores. Over time, chronically elevated cortisol promotes visceral fat accumulation around the abdomen, worsening systemic inflammation and further degrading sleep architecture in a cascading loop.
The weight-to-sleep pathway operates through mechanical as much as hormonal routes. Excess adipose tissue is not confined to the body's surface — it accumulates internally, including within the walls of the upper airway. Fat deposits in the throat and tongue narrow the pharynx, making it prone to collapse during sleep, particularly in REM sleep when the muscles that support the airway are temporarily paralysed.
Central obesity — fat concentrated around the abdomen — adds pressure on the diaphragm, the primary breathing muscle during REM sleep. This combination produces the defining pattern of obstructive sleep apnea: repeated partial or complete airway collapse, oxygen saturation drops, and micro-arousals that prevent restorative deep sleep. A healthy blood oxygen saturation sits above 90%; in severe untreated OSA, it can drop into the 70s.
Obesity and sleep disruption are not parallel problems. They are the same problem viewed from opposite angles — each making the other more resistant to treatment.
Each micro-arousal fires its own cortisol spike — which, as described above, drives appetite, promotes fat retention, and worsens insulin resistance. The person wakes exhausted, gravitates toward calorie-dense food for energy, exercises less, and gains more weight — making the next night's sleep worse still. This is the literal, documented physiology of the vicious cycle.
Sleep deprivation impairs the prefrontal cortex — the brain region governing impulse control, decision-making, and evaluation of long-term consequences. Studies consistently find that sleep-deprived people show heightened neural reactivity to high-fat and high-sugar food stimuli, while the inhibitory circuits that ordinarily curb those cravings become significantly less effective.
Sleep loss also extends the eating window. More hours awake, combined with elevated hunger hormones and impaired self-regulation, produces what researchers call extended nocturnal eating. Food consumed late at night is metabolised less efficiently than food consumed during daylight hours — contributing to weight gain independently of total caloric intake.
For shift workers, this is especially acute. Rotating schedules disrupt the circadian clock — the internal timing system governing metabolism, hormone release, and the sleep-wake cycle. Research from the Sleep Health Foundation confirms that shift work elevates obesity and type 2 diabetes risk through precisely this disruption to circadian-regulated eating and metabolic processing.
Clinicians at UT Southwestern and elsewhere find that addressing sleep is often the fastest route to early progress in weight management. CPAP therapy — the gold-standard treatment for OSA — reduces apnea events per night, restores restorative sleep stages, and modestly lowers blood pressure. Accumulating evidence shows that improved sleep quality partially restores the hormonal balance that makes dietary discipline achievable.
Weight loss directly reduces OSA severity. Even a 10% reduction in body weight can meaningfully decrease the number of apnea events per night, improving overnight oxygenation and sleep continuity. The relationship is dose-dependent — greater weight loss yields greater improvement. This reciprocal benefit underpins clinical guidelines recommending weight management and sleep therapy be pursued concurrently, not sequentially.

The findings and claims throughout this article draw from peer-reviewed literature and accredited institutional health sources. Key references are listed below.
Credibility note: This article synthesises findings from peer-reviewed clinical literature and accredited institutional health authorities. It is intended for informational purposes only and does not constitute medical advice. Individuals with concerns about sleep disorders or weight should consult a qualified healthcare professional.
This article was produced by the Bloorian editorial team and draws on peer-reviewed scientific literature and expert clinical commentary from accredited medical institutions — including Brown University Health, UT Southwestern Medical Center, and the Sleep Health Foundation of Australia. No commercial relationships influenced the selection of sources or the framing of findings.
All statistical claims reference source material current as of mid-2025. Medical understanding of the sleep-obesity relationship continues to evolve; readers are encouraged to consult updated clinical guidelines and their own healthcare providers for personalised guidance.
Written by
MedBary Team
Comments
Log in to join the conversation.
Loading comments…