
When Antibiotics Fail: The Hidden Force Driving Peri-Implantitis
Dental implants have a well-earned reputation for durability — but for up to one in five recipients, a destructive jawbone infection called peri-implantitis undoes that success. Antibiotic regimens that reliably resolve similar infections around natural teeth consistently fall short here. A landmark 2026 study from Rutgers University has finally uncovered why — and the culprit is the implant itself.

Dental implants have a well-earned reputation for durability — but for up to one in five recipients, a destructive jawbone infection called peri-implantitis undoes that success. Antibiotic regimens that reliably resolve similar infections around natural teeth consistently fall short here. A landmark 2026 study from Rutgers University has finally uncovered why — and the culprit is the implant itself.
Why It Matters
A Puzzle That Has Resisted Two Decades of Research
Peri-implantitis initially resembles periodontitis — an infection triggered by the same oral bacteria, presenting with the same signs of inflammation. The logical expectation is that identical antibiotic protocols should work equally well. They do not. Clinicians have observed this therapeutic gap for years, but the biological reason behind it remained unknown.
Understanding this gap matters considerably. Over 350,000 implants placed annually go on to develop peri-implantitis. Advanced cases require flap surgery, surface decontamination, regenerative intervention, or complete implant removal — with unpredictable outcomes and substantial costs. For patients, the condition brings pain, suppuration, impaired chewing, and significant anxiety.
The new Rutgers-led findings fundamentally reframe the condition: peri-implantitis is not simply a harder-to-treat version of gum disease. It is a materially distinct immunological crisis, driven by the implant substrate itself.
Detailed Viewpoint
Inside the Immune Breakdown: From Corrosion to Bone Loss
The Rutgers team, led by Dr. Georgios Kotsakis — assistant dean for clinical research at the Rutgers School of Dental Medicine — conducted their investigation using human tissue samples, cultured immune cells, and a genetically engineered mouse model. Their findings, published in the April 2026 issue of PNAS Nexus, describe a cascade that begins not with a pathogen, but with metal corrosion.
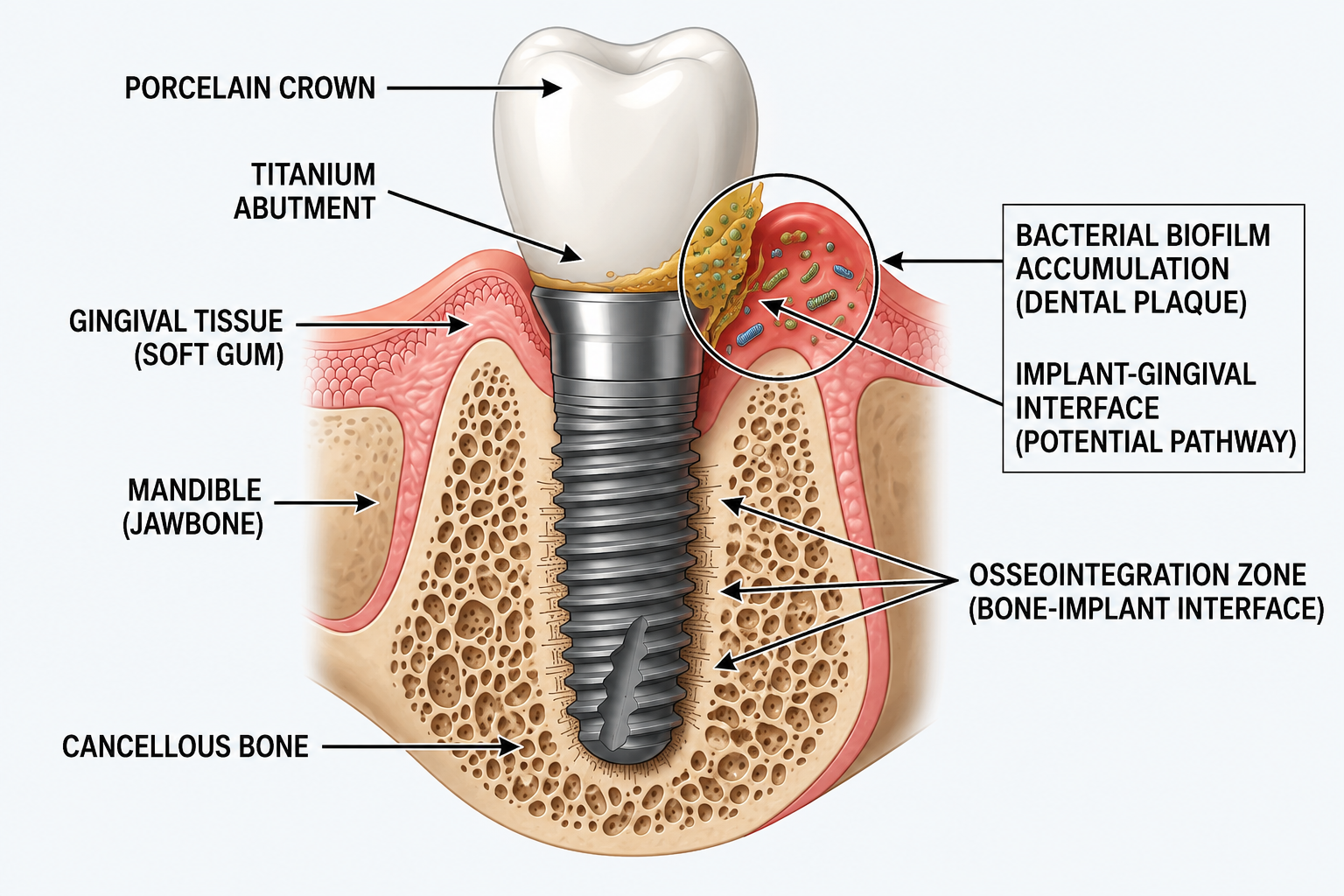
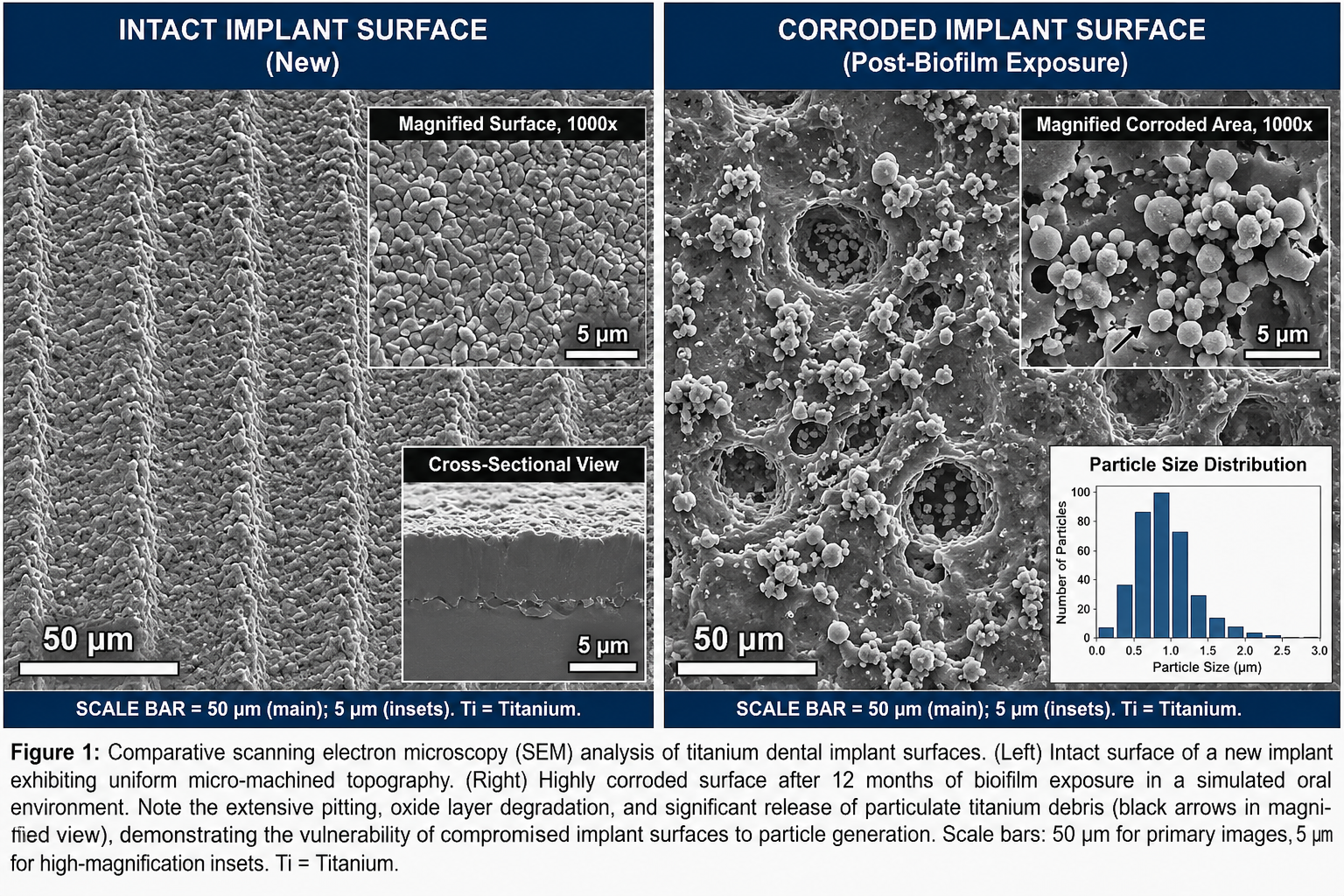
Biofilm forms and corrodes the implant surface. Bacteria colonize titanium implants rapidly through a process sometimes called the "race for the surface." Their acidic biofilms slowly corrode the titanium, releasing billions of particles smaller than a red blood cell into the surrounding peri-implant tissue. This shedding is also triggered by conventional metal scaling instruments used on implant surfaces during routine maintenance.
Titanium particles become coated in bacterial toxins. Inside gum tissue, the shed particles acquire a layer of lipopolysaccharide (LPS) — a potent bacterial toxin. To the immune system's pattern-recognition machinery, they suddenly resemble enormous, indigestible pathogens. The research team described them as "little magnets" that concentrate both the bacterial toxin and the immune response in one place.
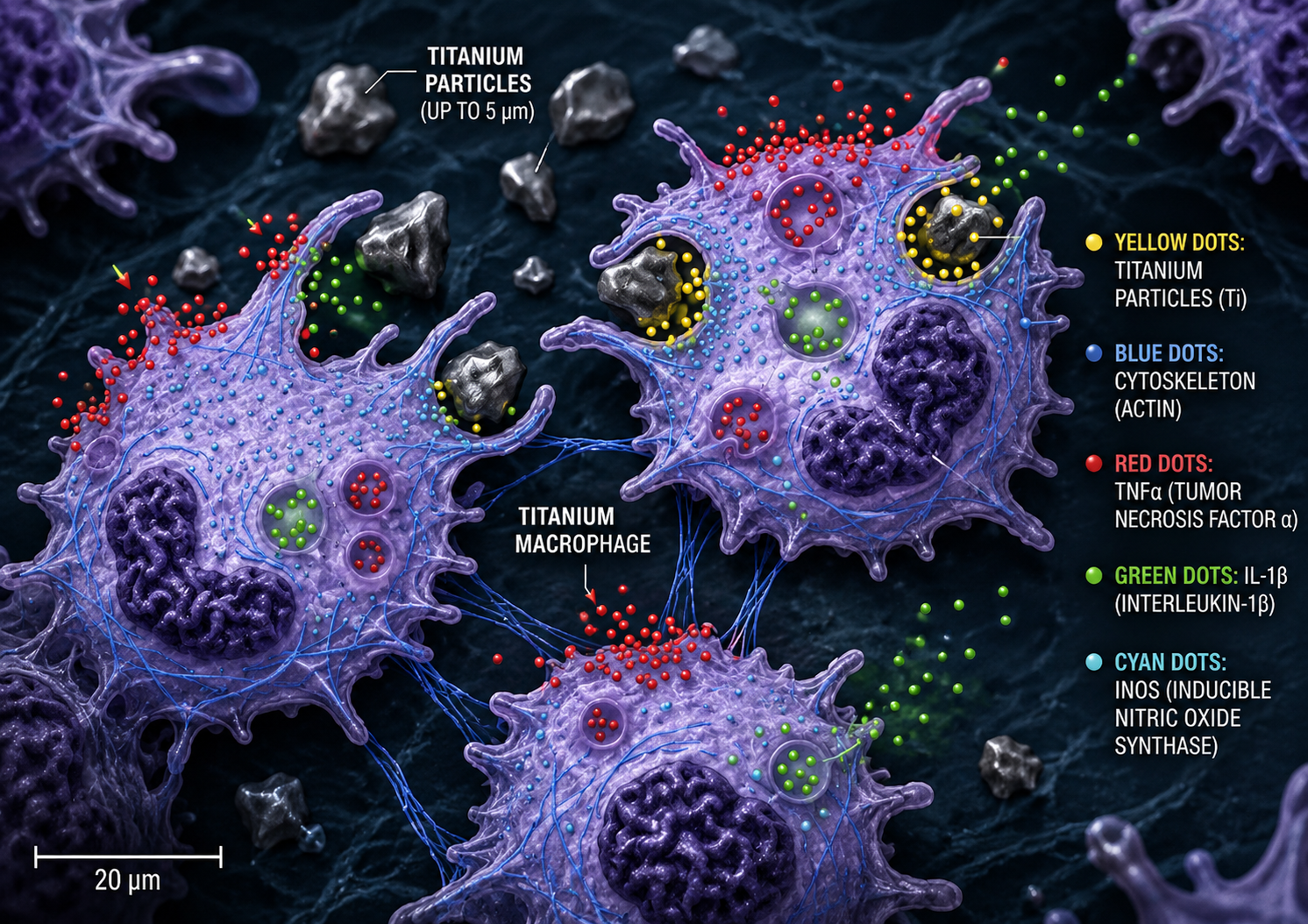
Macrophages engulf the particles but cannot clear them. Macrophages — the immune system's bacterial "vacuum cleaners" — engulf the toxin-coated particles. But they cannot digest metal. The study found that macrophages exposed to titanium particles cleared fewer than half as many bacteria as unexposed cells, disabling the immune mechanism that antibiotics rely on to finish the job.
TRPC1 locks macrophages into a hyperinflammatory state. The team traced the mechanism to a calcium channel called TRPC1 (transient receptor potential canonical 1). When titanium particles activate this channel, immune cells become trapped in a self-perpetuating inflammatory loop, releasing interleukin-1 beta — a cytokine also implicated in rheumatoid arthritis and Alzheimer's disease. In mice engineered without TRPC1, abscesses shrank dramatically, inflammatory markers dropped, and bacterial clearance was restored.
Chronic inflammation destroys bone rather than protecting it. The signaling cascade intended to recruit defenses instead consumes the supporting jawbone. Antibiotics — which target bacteria — cannot interrupt this materials-driven immunological process. This is precisely why the same drugs that resolve periodontitis fail against peri-implantitis: they address the wrong component of the disease entirely.
Emerging Solutions
Beyond Antibiotics: What the Science Points Toward
The identification of TRPC1 as the key mediator of macrophage dysfunction opens an entirely new therapeutic direction. Rather than targeting bacteria — which antibiotics already do imperfectly — future treatments may focus on modulating the inflammatory response itself. NIH-funded researchers at Rutgers are currently testing drug candidates that block the TRPC1 pathway in human cell cultures.
The first credible drug target for peri-implantitis. NIH-funded trials in human cells are ongoing (Rutgers, 2026).
Replacing metal scalers with plastic, carbon-fibre, or ultrasonic tips significantly reduces titanium particle release during maintenance visits.
AMP-coated titanium implants show promise in reducing early biofilm formation and slowing corrosion (Int. J. Dent., 2025).
Zirconia and ceramic implants are under investigation as corrosion-resistant alternatives that may generate fewer immunogenic particles.
On a clinical level, the single most actionable finding is reinforcement of proper maintenance protocol. The strongest known protective factor is regular professional cleaning but the instruments used matter critically. Use of metal scalers on implant surfaces can itself accelerate corrosion and particle release, compounding the very condition being treated.
Citations & Credibility
Kotsakis, G. et al. (2026). Implant-derived titanium particles impair macrophage bacterial clearance via TRPC1 and lysosomal dysfunction. PNAS Nexus, April 2026. NIH-funded; Rutgers School of Dental Medicine. academic.oup.com ↗
Smith, A. (May 28, 2026). Why Antibiotics Fail Against a Common Dental Implant Disease. Rutgers University News & Research. rutgers.edu ↗
Jazaeri, M. et al. (2025). Biofilm removal capacity and titanium surface integrity in non-abrasive versus abrasive peri-implantitis cleaning interventions. Journal of Periodontology. Provides $2.3B 2024 cost estimate. onlinelibrary.wiley.com ↗
Saleh, M. et al. (2025). Preventing peri-implantitis: strategies, mechanisms, and clinical perspectives for inhibiting biofilm formation on implant surface. Frontiers in Materials, 12, 1739290. frontiersin.org ↗
Kotsakis, G.A. & Ganesan, S.M. (2025). Microbial Dysbiosis, Titanium Release, and Peri-implantitis. Journal of Dental Research. journals.sagepub.com ↗
Liu, X. et al. (2025). Effectiveness of a Local Drug Delivery System Based on Antimicrobial Peptides in Early Treatment of Peri-implantitis. Int. Journal of Dentistry, 75(2). sciencedirect.com ↗
Dental Tribune (June 5, 2026). Titanium particles linked to antibiotic failure in peri-implantitis. dental-tribune.com ↗
All cited studies are peer-reviewed and published in indexed journals. The primary research (Ref. 1) was funded by the National Institutes of Health (NIH) and conducted at the Rutgers School of Dental Medicine. Cost figures are drawn from the Journal of Periodontology (2025) systematic assessment. This article is for informational purposes; patients and clinicians should consult current clinical guidelines.
Written by
MedBary Team
Comments
Log in to join the conversation.
Loading comments…