
Healthcare Business Models: Fee-for-Service to Value-Based Care
Healthcare business models are shifting from volume-driven reimbursement toward payment structures that reward quality, outcomes, efficiency, and coordinated care. Fee-for-service remains deeply embedded in healthcare finance, but value-based care is changing how hospitals, physicians, payers, and investors think about growth, risk, data, and long-term sustainability.


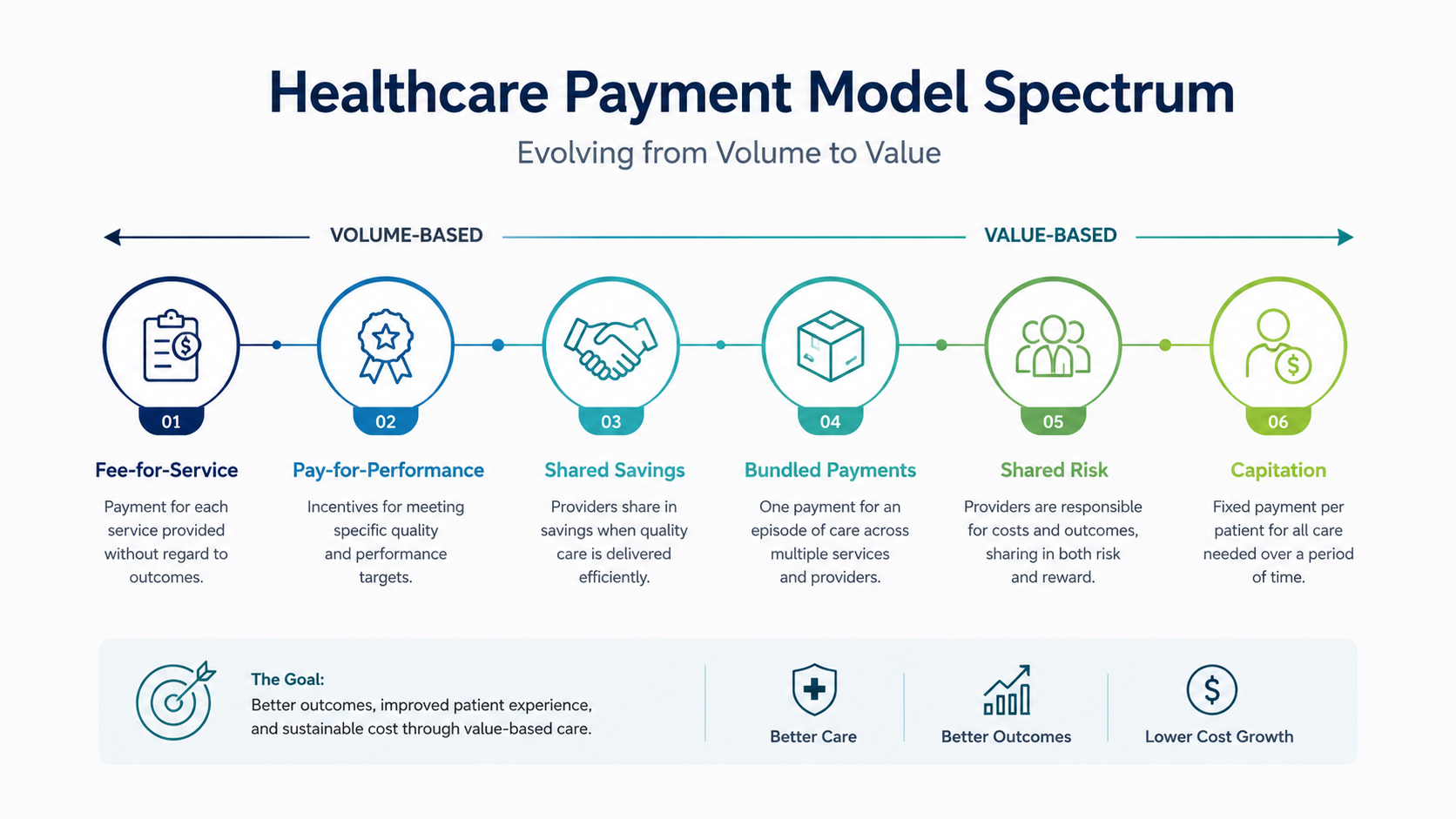
The business model is shifting from volume, to value, to managed risk
Fee-for-service rewards volume
Traditional payment models generate revenue when visits, tests, procedures, admissions, and billable services increase.
Value-based care rewards results
Value-based models tie payment to quality, outcomes, patient experience, population health, and total cost performance.
Risk changes management
When providers accept shared savings, shared losses, bundled payments, or capitation, finance and clinical operations become inseparable.
Data becomes infrastructure
Organizations need accurate attribution, cost accounting, quality measurement, care-gap analytics, claims data, and risk adjustment.
Hybrid models dominate
Most providers operate in mixed reimbursement environments where fee-for-service and value-based contracts coexist.
Execution decides success
The winners will be organizations that align physicians, care teams, technology, finance, quality, and patient access around the same model.
Payment models shape almost every operational decision in healthcare.
The way healthcare organizations are paid affects what they build, how they staff, where they invest, how they manage referrals, and which services receive executive attention. Fee-for-service models reward activity: more visits, tests, procedures, admissions, and billable encounters. Value-based models reward performance: better outcomes, fewer avoidable complications, stronger care coordination, and lower total cost.
The pressure to rethink healthcare payment is not theoretical. U.S. national health spending reached $5.3 trillion in 2024, representing 18.0 percent of GDP, according to CMS [1]. At that scale, even small changes in payment incentives can shift billions of dollars across hospitals, physicians, payers, employers, and patients.
The strategic challenge is that healthcare is not moving cleanly from one model to another. Most organizations must manage a hybrid environment: fee-for-service revenue still funds operations, while value-based contracts require investment in prevention, analytics, access, chronic disease management, and care coordination. The business model is becoming more complex, not less.
From billing more services to managing total value
For decades, the dominant healthcare business model has been fee-for-service. Under this structure, providers are paid when they deliver a billable service. A consultation, diagnostic test, procedure, admission, therapy session, imaging study, or follow-up visit becomes a revenue event. The model is relatively easy to understand, aligns with traditional billing systems, and gives hospitals and physicians a clear link between service volume and revenue.
But fee-for-service also creates a difficult incentive problem. It rewards activity more directly than outcomes. A hospital may be paid for complications, readmissions, duplicated tests, and avoidable utilization, even though those events are bad for patients and expensive for the system. This does not mean clinicians intentionally deliver unnecessary care. It means the business model can make prevention, coordination, and long-term population health financially harder to prioritize.
1. Fee-for-service is simple, powerful, and still deeply embedded
Fee-for-service remains attractive because it is transactional. Revenue is tied to identifiable services, charges, codes, contracts, and claims. This makes it easier to forecast revenue from surgical volume, imaging utilization, clinic visits, emergency department encounters, and inpatient admissions. It also supports specialty growth strategies because higher-acuity procedures and procedural service lines can generate meaningful contribution margin.
Many hospital departments were built around this logic. Operating rooms, imaging centers, cath labs, endoscopy suites, specialty clinics, laboratory outreach programs, and emergency departments often depend on throughput. Leaders track utilization, payer mix, cost per case, charge capture, denial rates, scheduling efficiency, and contribution margin. These measures are still essential, especially where fee-for-service contracts remain dominant.
The problem is not that fee-for-service is useless. The problem is that it is incomplete. A model that pays mainly for activity may underpay the work required to keep people healthier, avoid unnecessary utilization, coordinate between providers, manage social risk, or support patients after discharge.
2. Value-based care changes the definition of performance
Value-based care attempts to rebalance incentives. CMS describes value-based programs as payment approaches that reward providers for quality rather than only quantity, supporting better care, better population health, and lower cost [2]. In practical terms, this means healthcare organizations may receive bonuses, penalties, shared savings, or risk-based payments depending on how well they manage outcomes and total cost.
These models can take several forms. Pay-for-performance adds quality incentives to traditional reimbursement. Shared-savings contracts allow providers to share in savings if total spending comes in below a benchmark while quality targets are met. Shared-risk models expose providers to losses if spending exceeds targets. Bundled payments set a single payment for an episode of care, such as joint replacement or cardiac surgery. Capitation pays a fixed amount per member over a defined period, shifting greater responsibility for cost and outcomes to the provider organization.
The deeper shift is cultural. Under fee-for-service, the question is often, “How many services did we provide?” Under value-based care, the question becomes, “Did we improve health outcomes at an appropriate total cost?” That question changes how executives think about patient access, primary care, care management, analytics, physician alignment, and post-acute partnerships.
3. The transition is not one model replacing another overnight
The most common mistake is assuming healthcare is simply “moving from fee-for-service to value-based care.” In reality, most organizations are operating in both worlds at once. One contract may reward admissions and procedures. Another may penalize readmissions. One payer may pay per service. Another may use bundled payments or shared savings. Medicare, Medicaid, commercial insurers, employers, and self-pay patients may all create different incentives inside the same organization.
This hybrid reality creates strategic tension. A hospital may lose fee-for-service revenue when it successfully reduces avoidable admissions, even if the same effort improves value-based performance. A primary care investment may reduce emergency department utilization, but the financial benefit may go to the payer unless the provider participates in shared savings or risk contracts. A care-management program may improve outcomes but require upfront staffing and technology expense before returns are visible.
Leaders therefore need contract-level clarity. They should know which patient populations are attributed to value-based contracts, which services remain fee-for-service, where incentives conflict, and which investments benefit both models. Without this clarity, organizations may underinvest in value-based capabilities or unintentionally damage their own revenue base.
4. Risk requires new operating capabilities
Taking financial risk is not simply a contracting decision. It is an operating model decision. A provider accepting downside risk must be able to identify attributed patients, understand disease burden, close care gaps, manage high-risk members, coordinate across settings, control avoidable utilization, and document conditions accurately. Weak data, poor access, fragmented care, or delayed follow-up can turn a promising risk contract into a financial liability.
This is why value-based care often requires investment in primary care, care management, analytics, patient outreach, pharmacy support, behavioral health integration, home health partnerships, post-acute networks, and social-needs navigation. These capabilities are not always revenue-generating in a traditional fee-for-service sense. Their value comes from preventing avoidable cost, improving outcomes, and earning incentive payments or shared savings.
The Health Care Payment Learning & Action Network tracks the movement of health care payments into alternative payment models and emphasizes the shift toward models tied to quality, value, and two-sided risk [3]. For executives, this means the question is no longer whether alternative payment models exist. The question is how prepared the organization is to perform under them.
5. Physician alignment is the center of the model
No payment model works without physician alignment. In fee-for-service, alignment often focuses on referral patterns, productivity, scheduling, procedural volume, and clinical documentation. In value-based care, alignment expands to include quality measures, care coordination, medication adherence, preventive screening, patient access, risk adjustment, appropriate specialist use, and total cost of care.
Compensation models must evolve carefully. Paying physicians only for productivity can undermine value-based goals. Paying only for quality can create dissatisfaction if workload and patient complexity are not recognized. Strong models usually blend productivity, panel management, quality, access, patient experience, documentation, and team-based care expectations.
Governance also matters. Physicians should not experience value-based care as a finance project imposed from above. They need transparent data, fair benchmarks, clinical leadership, workflow support, and meaningful input into measure design. The more risk an organization takes, the more important physician trust becomes.
6. Hospitals need a portfolio strategy, not a slogan
The best healthcare organizations do not treat value-based care as a branding phrase. They build a portfolio strategy. Some service lines may remain primarily fee-for-service for years. Others may be suited to bundled payments. Primary care, chronic disease management, Medicare Advantage, accountable care, employer partnerships, and post-acute networks may be better suited to population-based or risk-based models.
A portfolio view helps leaders decide where to invest. Fee-for-service service lines still require throughput, access, revenue-cycle discipline, referral development, and cost control. Value-based populations require risk stratification, care-gap closure, patient engagement, utilization management, and longitudinal outcomes. Both require accurate data and strong clinical quality.
The future healthcare business model will not belong to organizations that simply abandon fee-for-service or blindly accept risk. It will belong to organizations that understand incentives, price risk correctly, build operational capability before taking major downside exposure, and align care delivery with the payment model they are trying to win.
Sources used for context
Editorial Note: This article is produced for informational and educational purposes. It does not constitute financial, legal, clinical, regulatory, or reimbursement advice. Healthcare organizations should evaluate payment models, risk contracts, compliance obligations, and operational strategies with qualified advisors, legal counsel, clinical leadership, and finance teams before making business or care-delivery decisions.
Written by
MD Zee
Comments
Log in to join the conversation.
Loading comments…