
Triage Systems and Their Impact on Hospital Revenue
Emergency-department triage is primarily a clinical safety function, but its design also affects patient flow, staffing efficiency, diagnostic utilization, admission decisions, patient abandonment, and hospital revenue. The strongest triage models protect clinical priority while moving each patient into the right care pathway as early as possible.

Six ways triage influences emergency-department economics
Earlier prioritization protects capacity
Accurate acuity classification helps high-risk patients receive rapid treatment while lower-acuity patients move to appropriately designed pathways.
Long waits create lost demand
Patients who leave before evaluation or treatment represent missed care, potential safety risk, reduced revenue, and weaker community confidence.
Routing affects resource cost
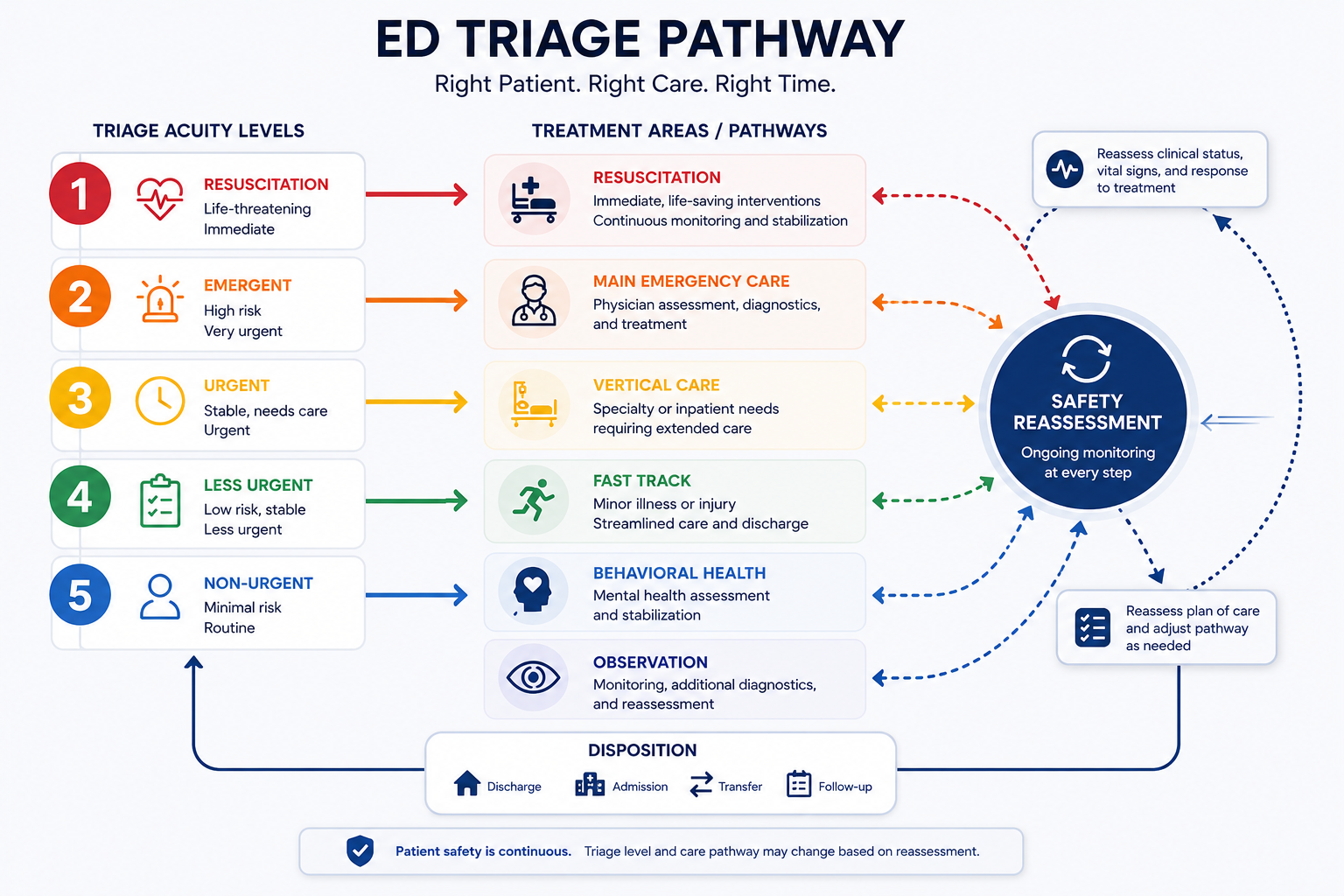
Fast-track, vertical-care, resuscitation, observation, behavioral-health, and main-treatment pathways require different staffing and space.
Documentation supports payment
Reliable triage documentation supports continuity, medical necessity, severity recognition, handoffs, quality review, and accurate coding.
Triage cannot solve boarding alone
Emergency flow will remain constrained when admitted patients cannot move to inpatient beds or suitable post-acute settings.
Data should guide redesign
Arrival patterns, acuity, door-to-provider time, abandonment, length of stay, admissions, staffing, and contribution margin should be reviewed together.
Triage is the clinical front door to one of the hospital’s most complex operating environments.
U.S. emergency departments recorded an estimated 155.4 million visits in 2022, including approximately 17.8 million visits that resulted in hospital admission [1]. At that scale, small differences in assessment speed, patient routing, staffing, documentation, and treatment initiation can produce significant effects on capacity and financial performance.
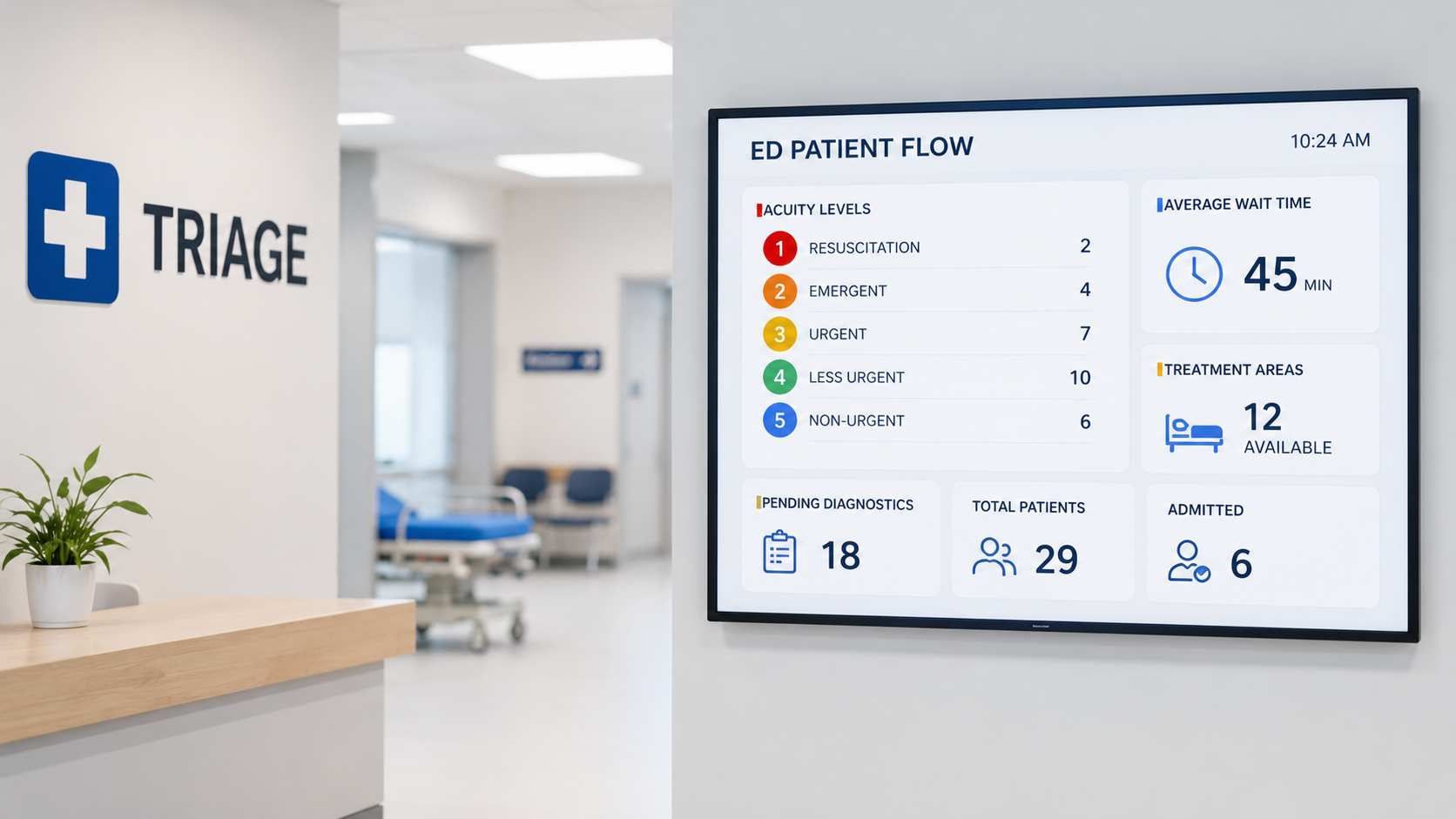
AHRQ describes the Emergency Severity Index as a five-level triage system that classifies patients from Level 1, the most urgent, to Level 5, the least urgent, using both clinical acuity and anticipated resource needs [2]. This makes triage more than a waiting-room process. It is an early resource-allocation decision that influences which clinicians, beds, diagnostics, and treatment spaces a patient may require.
The financial objective cannot override the clinical purpose. Triage must first identify risk and support safe, equitable access to emergency evaluation. In the United States, EMTALA requires Medicare-participating hospitals with emergency services to provide an appropriate medical screening examination when emergency evaluation or treatment is requested, regardless of a person’s ability to pay [3]. Revenue improvement must therefore come from safer flow and better operations—not from restricting access or diverting patients based on insurance status.
Triage creates financial value when it moves patients safely into the right care process
Emergency-department triage is sometimes viewed as an administrative queue: patients arrive, receive a category, and wait until a treatment space becomes available. That description misses its strategic value. Triage is the first structured clinical decision in the emergency-care journey. It identifies immediate threats, establishes priority, anticipates resource needs, supports reassessment, and helps determine where the patient should go next.
The revenue impact is indirect but substantial. A strong triage process can reduce avoidable delay, support earlier diagnostics, improve treatment-area utilization, reduce the number of patients who leave before care, strengthen documentation, and increase the number of patients the department can safely manage. A weak process creates bottlenecks, repeated assessments, poorly matched resources, safety events, patient abandonment, and preventable cost.
1. Acuity classification should protect both safety and capacity
The first responsibility of triage is to identify patients who cannot safely wait. Chest pain, stroke symptoms, severe respiratory distress, shock, major trauma, altered mental status, obstetric emergencies, sepsis indicators, and other time-sensitive presentations require rapid escalation. Missing urgency can cause patient harm, increase treatment complexity, extend length of stay, and expose the organization to legal and reputational consequences.
Over-triage also has consequences. When too many patients are assigned to the highest-acuity spaces, scarce beds, nurses, monitors, and physicians may be occupied by patients who could be managed safely in a lower-intensity area. Under-triage risks clinical deterioration. Over-triage creates inefficient resource use. The goal is not to classify patients in the most cautious category possible; it is to place them in the safest accurate category supported by the available evidence.
AHRQ’s Emergency Severity Index incorporates both urgency and expected resource needs [2]. That second dimension has operational importance. Two patients may appear clinically stable, but one may need laboratory tests, imaging, medication, specialist consultation, and possible admission, while the other may require a focused examination and simple treatment. Anticipating that difference allows the department to prepare capacity earlier.
2. Patient abandonment represents clinical and financial loss
Patients who leave before being seen or before treatment is complete are among the clearest examples of emergency-department demand that fails to convert into delivered care. Some leave because symptoms improve, but many leave because the perceived wait becomes unacceptable. Each departure may represent a missed opportunity for assessment, treatment, diagnostics, admission, referral, or follow-up.
The financial effect is broader than the unbilled emergency visit. A patient who leaves may seek care at a competing hospital, transfer future family utilization elsewhere, post a negative review, or return later with a more advanced condition. An older financial analysis of emergency-department boarding and lost demand found that patients leaving without being seen were associated with forgone revenue and that crowding could also constrain higher-value inpatient demand [4]. The precise dollar impact will differ by hospital, payer mix, case severity, and local market.
Triage redesign can help by reducing the time between arrival and meaningful clinical contact. Registration may be streamlined, a rapid visual assessment may occur immediately, and stable patients may move directly to an appropriate care zone. The objective is not to rush the clinical assessment. It is to remove nonclinical delay before assessment begins.
3. Split-flow pathways can use expensive resources more precisely
A single queue feeding a single type of treatment room is rarely the most efficient model for a high-volume emergency department. Patient needs differ too widely. A resuscitation patient needs immediate high-intensity care. A stable ambulatory patient may require a limited number of tests and treatments without occupying a stretcher. A behavioral-health patient may need a safe assessment environment. A patient awaiting a short period of monitoring may be appropriate for observation.
Split-flow models create different pathways based on patient condition, mobility, anticipated resources, and probable disposition. Common options include rapid assessment, fast track, vertical care, provider in triage, internal waiting, observation, and specialty-specific pathways. When matched to actual arrival patterns, these models can increase treatment capacity without requiring every patient to occupy a full emergency bed.
A study of a provider-in-triage model examined its effect on emergency length of stay and operational and financial outcomes, illustrating why organizations increasingly evaluate early-provider models as both patient-flow and business interventions [5]. However, adding a clinician to triage is not automatically profitable. The benefit depends on staffing cost, operating hours, volume peaks, available downstream capacity, and whether early orders actually shorten the care journey.
4. Earlier diagnostic activity must be governed carefully
Provider-in-triage and advanced triage protocols may allow laboratory tests, imaging, medication, or electrocardiography to begin earlier. This can shorten the interval between arrival and clinical decision-making, especially when treatment rooms are unavailable. Earlier completion of diagnostics may support faster discharge or admission once a main clinician evaluates the patient.
The financial risk is unnecessary utilization. Broad order sets used without sufficient clinical judgment may generate tests that do not change treatment or disposition. Duplicate orders can occur when the main treatment team repeats work initiated at triage. Organizations therefore need carefully designed protocols, defined eligibility criteria, order visibility, feedback to clinicians, and regular review of diagnostic yield.
Revenue should not be increased by ordering more services solely because they are billable. The sustainable opportunity is to begin medically necessary care earlier, remove duplication, and shorten avoidable waiting. The best financial result often comes from using fewer resources more deliberately rather than increasing the number of tests per patient.
5. Documentation connects triage with quality and revenue integrity
High-quality triage documentation records the presenting concern, relevant history, vital signs, pain or distress, risk factors, acuity decision, immediate interventions, reassessment requirements, and escalation. This record supports the clinical team’s understanding of how the patient presented and how the condition changed while waiting.
Documentation also supports coding, quality measurement, medical-necessity review, utilization management, denial prevention, and legal review. Missing or contradictory information can weaken the record even when appropriate care was provided. Triage nurses and clinicians should understand that structured documentation is not merely a compliance task. It is part of the hospital’s clinical and financial evidence.
Standardization should not eliminate professional judgment. Templates should make essential information easier to capture without encouraging superficial copying or irrelevant documentation. Leaders should audit both completeness and usefulness.
6. Triage is not a substitute for hospital-wide patient flow
A hospital can improve front-end triage and still experience severe emergency crowding if admitted patients remain in the department. Boarding occurs when the decision to admit has been made but an inpatient bed or appropriate placement is unavailable. These patients continue using emergency beds, nursing attention, monitoring, and operational capacity even though their emergency evaluation is complete.
AHRQ’s patient-flow guidance treats emergency crowding as a hospital-wide challenge rather than an emergency-department problem alone [6]. Inpatient discharge timing, environmental services, bed assignment, specialist decisions, transport, diagnostic turnaround, pharmacy, post-acute availability, and executive escalation all influence whether emergency capacity becomes available.
This distinction matters financially. Adding triage staff may improve early assessment, but it cannot create inpatient beds. Opening a fast-track area may improve lower-acuity flow, but it will not solve prolonged boarding of admitted patients. Investment decisions should be based on the true location of the constraint.
7. Staffing should follow demand patterns rather than fixed tradition
Emergency arrivals vary by hour, day, season, community events, weather, respiratory illness, and local service availability. Staffing based mainly on historical shift structures may create periods of excess capacity followed by severe mismatch during predictable peaks.
Triage analytics should show arrivals in short intervals, acuity distribution, ambulance arrivals, behavioral-health demand, pediatric patterns, diagnostic requirements, admission probability, and average treatment time. These data can inform when additional triage nurses, advanced-practice clinicians, physicians, technicians, registrars, transport staff, or environmental-services personnel are most valuable.
The lowest-cost staffing model is not necessarily the most efficient. Reducing staffing during a high-demand period may create waits, abandonment, overtime, delayed admissions, and patient-safety concerns that cost more than the avoided labour expense. The correct question is whether each added staffing hour creates sufficient clinical and operational value.
8. Build one dashboard for safety, flow, and financial performance
Triage performance should not be judged by one metric. A very short triage time may look efficient while hiding rushed assessments. A low abandonment rate may coexist with excessive total length of stay. Higher visit volume may create little value if staffing costs, denials, unnecessary testing, or admission delays rise faster than revenue.
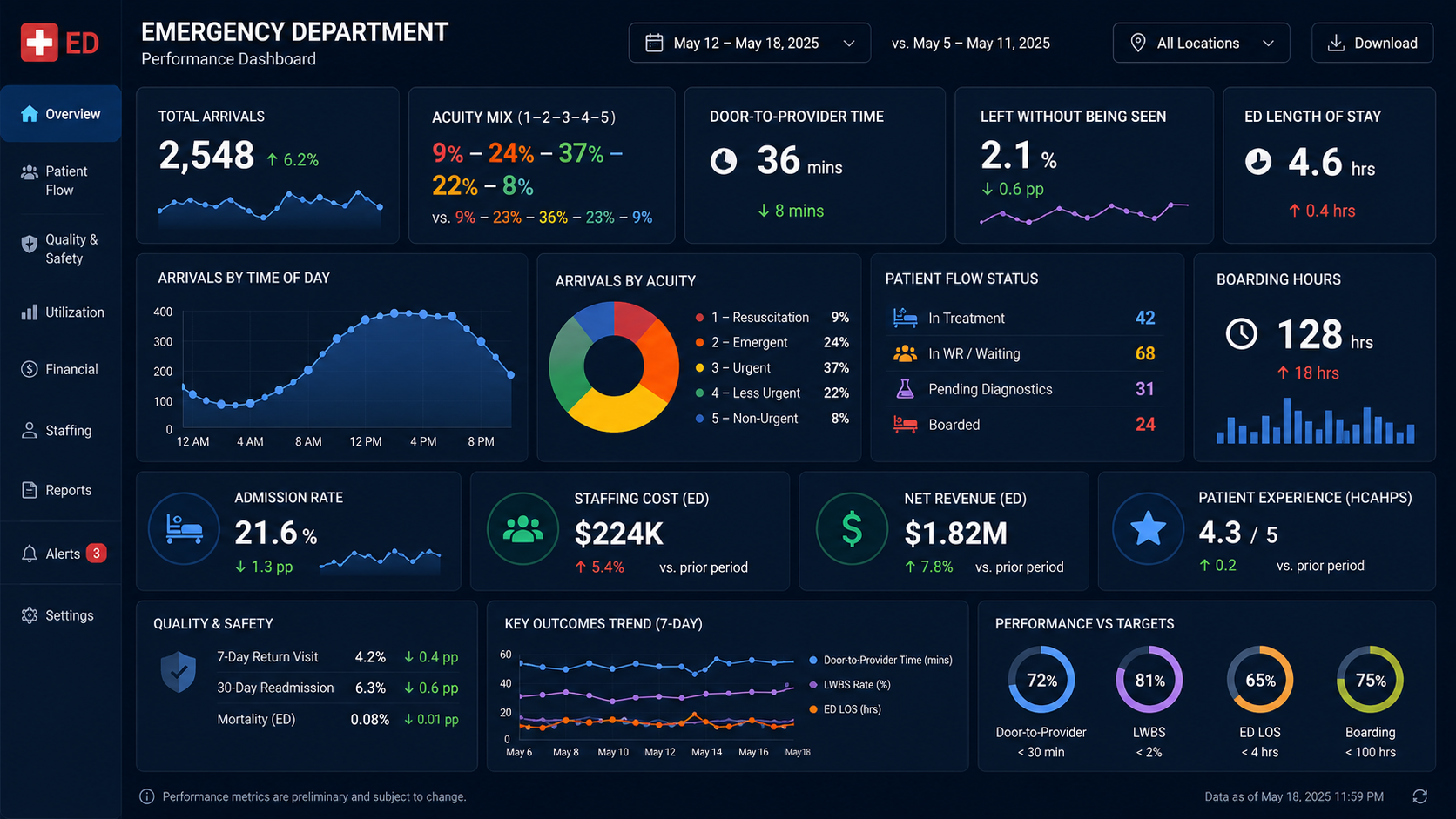
A balanced emergency dashboard should include arrival-to-triage time, door-to-clinician time, time-sensitive treatment measures, reassessment compliance, left-without-being-seen rate, patients leaving before treatment completion, emergency length of stay, boarding time, admission conversion, diagnostic turnaround, staffing hours, payer mix, net revenue per visit, denial rates, and contribution margin.
Performance should also be reviewed by acuity, age, language, race and ethnicity where legally and operationally appropriate, arrival mode, behavioral-health status, and other relevant patient characteristics. A financially efficient triage model that creates unequal access or misses high-risk patients is not a successful model. The strongest system improves safety, equity, experience, throughput, and financial sustainability together.
Sources used for context
Editorial Note: This article is intended for informational and educational purposes only. It does not constitute legal, financial, billing, reimbursement, clinical, operational, or regulatory advice. Triage systems, revenue-cycle workflows, coding practices, staffing models, and emergency-department protocols should be evaluated within each hospital’s jurisdiction, payer requirements, clinical governance standards, and patient-safety obligations. Healthcare leaders should consult qualified clinical, compliance, finance, coding, legal, and operational experts before making decisions that affect triage design, billing processes, care delivery, or hospital revenue strategy.
Written by
MD Zee
Comments
Log in to join the conversation.
Loading comments…