Apixaban vs Rivaroxaban: Rethinking the Default Choice in VTE Anticoagulation
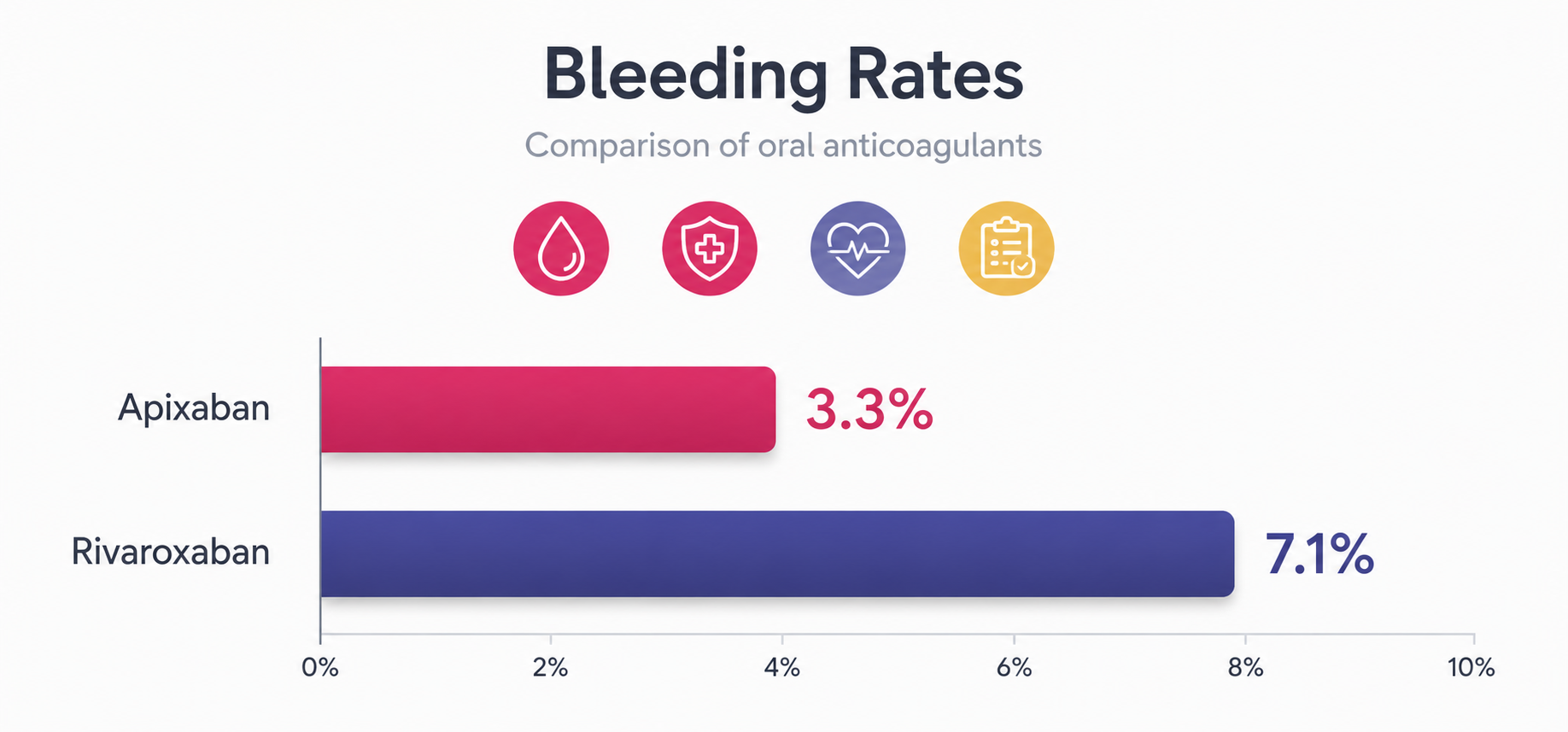
For years, apixaban and rivaroxaban have been treated as interchangeable workhorses of venous thromboembolism (VTE) management. Both are direct oral anticoagulants (DOACs), both target Factor Xa, and both outperform warfarin in landmark trials. But the landmark 2026 COBRRA trial now places a crucial wedge between them: apixaban produced clinically relevant bleeding in just 3.3% of patients compared to 7.1% with rivaroxaban over three months — a statistically significant difference that reshapes how clinicians should approach first-line anticoagulant selection.


Key Highlights
Apixaban clinically relevant bleeding rate in COBRRA — versus 7.1% for rivaroxaban
Patients randomized in the international COBRRA RCT — the first head-to-head trial for acute VTE
Lower relative risk of bleeding with apixaban — RR 0.46 (95% CI 0.33–0.65, p<0.001)
Rivaroxaban's loading window (15 mg BID) where excess bleeding clusters — apixaban's 7-day load avoids this
VTE recurrence in both arms — confirming equivalent efficacy while apixaban wins on safety
Covered in the UBC TI meta-analysis (42 cohort studies) — apixaban safer in AF populations too
Why It Matters
Massive Patient Population
VTE causes an estimated 60,000–100,000 deaths annually in the US alone. With apixaban and rivaroxaban as the two dominant DOACs, even a modest bleeding-risk difference translates to a substantial number of preventable adverse events at the population scale.
First Direct Head-to-Head RCT
Until COBRRA, drug selection rested on indirect evidence and observational data. A properly randomized, international, blinded-endpoint trial (2,760 patients) now provides Level I evidence. The result was not marginal — apixaban's relative risk of bleeding was 0.46 versus rivaroxaban.
Dosing Architecture Is the Culprit
Rivaroxaban's VTE protocol requires 15 mg twice daily for 21 days before stepping down. This sustained loading phase is where excess bleeding accumulates. COBRRA data show bleeding clustered heavily in the rivaroxaban arm during those first 21 days — pointing to a structural pharmacological issue, not inherent molecular toxicity.
Consistent Across Indications
The safety advantage isn't limited to VTE. A UBC TI meta-analysis of 42 cohort studies (2.9 million AF patients) found apixaban associated with 38% lower major bleeding risk versus rivaroxaban, plus lower intracranial hemorrhage and total mortality — making the signal consistent and compelling.
Detailed Viewpoint
The COBRRA Trial: What the Data Actually Show
Published in the New England Journal of Medicine in March 2026, COBRRA (NCT04642430) is a prospective, randomized, open-label, blinded-endpoint international study that enrolled 2,760 patients with acute symptomatic pulmonary embolism or proximal deep vein thrombosis. Patients were randomized 1:1 to apixaban (n=1,370) or rivaroxaban (n=1,390) for three months at guideline-concordant doses.
The apixaban arm received 10 mg twice daily for 7 days, then 5 mg twice daily. The rivaroxaban arm received 15 mg twice daily for 21 days, then 20 mg once daily. The mean patient age was 58.3 years; 52.2% had DVT and 47.8% had PE (with or without DVT). The trial enrolled patients across Canada, Australia, Ireland, Switzerland, and the United States.
| Outcome | Apixaban | Rivaroxaban |
|---|---|---|
| Clinically relevant bleeding (primary) | 3.3% (44/1,345) | 7.1% (96/1,355) |
| Major bleeding (Hgb drop ≥2 g/dL or transfusion) | 0.4% (5) | 2.4% (32) |
| VTE recurrence | 1.1% (15) | 1.0% (14) |
| Death from any cause | 0.1% (1) | 0.3% (4) |
| GI bleeding | 0.6% | 1.0% |
Source: Castellucci LA et al., N Engl J Med. 2026;394(11):1051–1060. doi:10.1056/NEJMoa2510703
Understanding the Pharmacological Difference
Both drugs inhibit Factor Xa, but their pharmacokinetic profiles and dosing architectures differ meaningfully. Apixaban has a shorter half-life (~12 hours) and is dosed twice daily throughout therapy without an intensified loading phase. Its VTE protocol starts at 10 mg BID for 7 days — a brief, moderate load — before stepping to 5 mg BID.
Rivaroxaban has a longer half-life and is taken once daily at maintenance, but its VTE protocol involves 15 mg twice daily for a full 21 days — creating a sustained period of elevated anticoagulant intensity. COBRRA data show bleeding events clustered more heavily in the rivaroxaban arm during this loading window, suggesting the dosing regimen itself — not inherent molecular toxicity — is the primary driver of the safety gap.
"Rivaroxaban's 21-day loading phase may represent a period of pharmacologically unnecessary anticoagulant intensity — one that apixaban's regimen simply does not impose on the patient."
Beyond VTE: The Atrial Fibrillation Evidence Base
The safety signal favouring apixaban predates COBRRA. A 2024 systematic review by the UBC Therapeutics Initiative analyzed 42 cohort studies encompassing approximately 2.9 million patients with non-valvular atrial fibrillation (NVAF). Meta-analysis of 27 studies (N=2,135,415) found apixaban associated with substantially lower major bleeding risk versus rivaroxaban (pooled RR 0.62, 95% CI 0.53–0.74), reduced intracranial hemorrhage (RR 0.76, 95% CI 0.68–0.85), and lower total mortality (RR 0.86, 95% CI 0.79–0.95).
A 2025 JACC analysis using the TriNetX Research Network examined 5-year outcomes in 744,829 propensity-matched AF patients. Rivaroxaban users had 17% higher all-cause mortality (OR 1.17, 95% CI 1.15–1.20), 12% higher major bleeding (OR 1.12), and 9% higher VTE (OR 1.09) — with no meaningful difference in ischemic stroke risk. A registry-based six-centre cohort in JACC: Advances (2025) further confirmed apixaban's favourable profile across both AF and VTE populations.
Implications Across Practice Settings
The convergence of randomized and real-world evidence creates a practical inflection point. Clinicians are no longer working from incomplete indirect comparisons — they now have a large, high-quality RCT to anchor drug selection discussions. Pharmacists are especially well-positioned to operationalize this evidence: flagging transitions from rivaroxaban during the high-risk 21-day window, counselling on adherence (apixaban's twice-daily dosing had slightly lower adherence in COBRRA — 65.7% vs 75.1% — a factor worth discussing openly), and helping patients understand that similar efficacy comes with meaningfully different safety profiles.
For patients with elevated baseline bleeding risk — older adults, those on NSAIDs or antiplatelet agents, or those with prior bleeding history — COBRRA provides a clinically grounded justification for preferring apixaban. The availability of generic formulations of both drugs (reducing prices ~75% in Canada in 2023) removes cost as a tiebreaker, allowing the safety data to take centre stage.
One important caveat: COBRRA enrolled patients with acute symptomatic VTE at low complication risk. Massive PE, cancer-associated thrombosis, antiphospholipid syndrome, and extremes of body weight were outside the studied population. Decisions for those groups remain more individualized. The evidence also does not yet fully address extended anticoagulation beyond three months, though ongoing observational data continue to trend favourably for apixaban.

Citation & Credibility
- Castellucci LA, Chen VM, Kovacs MJ, et al. Bleeding risk with apixaban vs rivaroxaban in acute venous thromboembolism. N Engl J Med. 2026;394(11):1051–1060. doi:10.1056/NEJMoa2510703. [PMID: 41812192] PRIMARY RCT
- UBC Therapeutics Initiative Drug Assessment Working Group. Apixaban is safer and more effective than rivaroxaban for non-valvular atrial fibrillation. Therapeutics Letter 146. February 2024. [Systematic review; N=2,936,126 across 42 cohort studies]
- Vignarajah A, Tan M, Thong J, et al. Apixaban versus rivaroxaban: 5-year outcomes in atrial fibrillation management. JACC. 2025;85(12 Suppl):61. doi:10.1016/S0735-1097(25)00541-8. [TriNetX propensity-matched cohort, N=744,829]
- Schaefer J, Errickson J, Kong X, et al. A comparison of outcomes with apixaban, rivaroxaban, and warfarin for atrial fibrillation and/or venous thromboembolism. JACC: Advances. 2025;4(5). doi:10.1016/j.jacadv.2025.101714. [Registry-based cohort, 6 centres]
- Centers for Disease Control and Prevention. Data and statistics on venous thromboembolism. CDC. Updated January 2025. Accessed June 10, 2026. cdc.gov/blood-clots.
- Creager MA, Barnes GD, Giri J, et al. 2026 AHA/ACC guideline for the evaluation and management of acute pulmonary embolism in adults. Circulation. 2026;153(12). doi:10.1161/CIR.0000000000001415.
Article Tags
Written by
MedBary Team
Comments
Log in to join the conversation.
Loading comments…