The Infection That Turns IBD From a Managed Condition Into a Medical Crisis
Inflammatory bowel disease demands a lifetime of careful immune management — and Clostridioides difficile has learned to exploit every gap in that strategy. With IBD patients facing five times the infection risk of the general population, and a treatment landscape where fighting one condition can actively worsen the other, this is the collision doctors dread and patients rarely see coming.

IBD patients face a five-fold greater risk of C. diff infection compared with the general population — based on a 556-patient Finnish cohort study.
Of IBD patients who contract C. diff experience recurrent infections — 67% of those within 90 days of the first episode.
Estimated US C. diff infections annually — with 12,800 deaths and 223,000 hospitalizations each year (CDC / JAMA Network Open).
Of IBD flares are triggered or worsened by a gastrointestinal infection — with C. diff among the most consequential culprits.
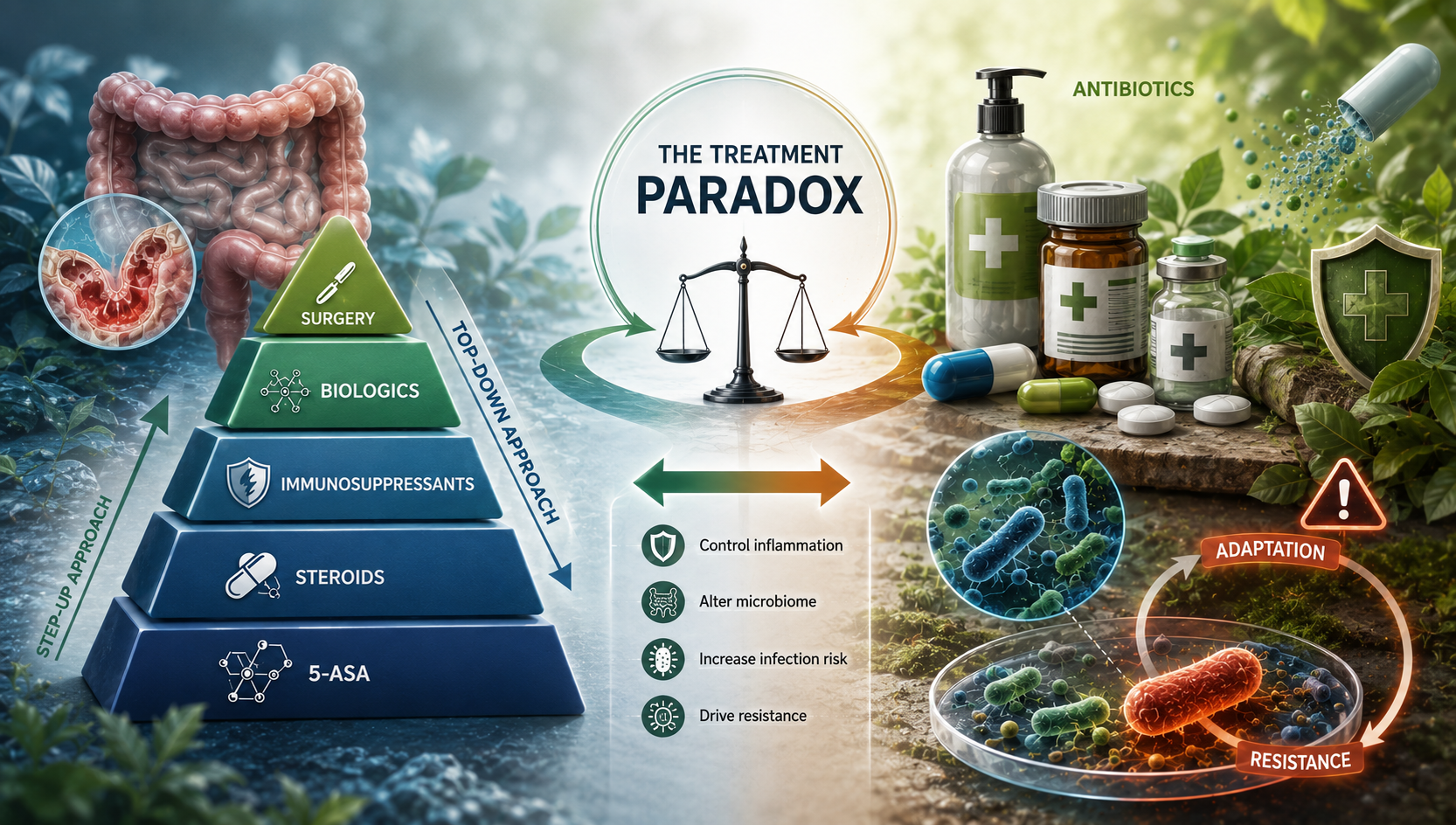
For someone already managing IBD — whether ulcerative colitis or Crohn's disease — a concurrent C. diff infection is far more than a complication. It strikes at the very heart of what makes IBD so difficult to treat: the need to modulate the immune system. IBD management frequently involves immunosuppressive therapies designed to calm an overactive immune response. But when C. diff enters the picture, those same treatments can create a window of vulnerability the bacterium is well-positioned to exploit.
The practical consequence is a clinical standoff. Escalating immunosuppression — the standard response to an IBD flare — can accelerate C. diff infection. Treating C. diff with antibiotics while maintaining full immunosuppression is equally fraught.
Beyond individual patient outcomes, the public health dimension is substantial. The CDC estimates C. diff causes close to half a million infections in the United States annually — 223,000 hospitalizations and 12,800 deaths — numbers that underscore why researchers from McMaster University to the University of Utah are devoting significant resources to understanding how the pathogen spreads.

What the Research Reveals
A retrospective Finnish cohort study examined 279 IBD patients with confirmed C. diff infection alongside 277 without. The median age at infection was just 37 years — considerably younger than typical C. diff demographics. IBD-associated C. diff is not a disease of the elderly; it strikes adults in their most productive decades.
Ulcerative colitis emerged as the dominant IBD subtype, accounting for 70% of infected patients — and 79% of those who experienced recurrent episodes, suggesting the UC mucosal environment is more hospitable to C. diff colonization.
Risk Factors Clinicians Need to Watch
Three factors consistently surfaced as predictors: active disease at the time of infection, a shorter duration since IBD diagnosis, and recent corticosteroid use. Advanced biologic therapies did not emerge as significant risk factors — a reassuring finding for patients on targeted treatments.
Corticosteroids suppress broad immune functions that leave the gut vulnerable. The CDC has documented that individuals are up to ten times more likely to develop C. diff during or within three months of antibiotic therapy — a compounding risk for IBD patients who cycle through antibiotics.
The Hidden Spread Problem in Healthcare Settings
A University of Utah study published in JAMA Network Open found that approximately 8% of admitted ICU patients had C. diff genetically linked to another patient — more than three times what standard surveillance detected. The methodology captured transmission events that entirely bypassed patient body-site testing.
Over a third of hospital-associated C. diff cases originate from asymptomatic carriers. McMaster University IIDR researchers applied whole-genome sequencing to isolates from four Ontario hospitals — mapping clonal spread and identifying which groups gave rise to active outbreaks, intelligence directly applicable to infection control design.
Treatment and the Path Forward
First-line treatment involves a 10-day course of vancomycin or fidaxomicin. In IBD patients this is layered by the concurrent need to manage disease activity — sometimes requiring immunosuppression reduction that can itself trigger a flare.
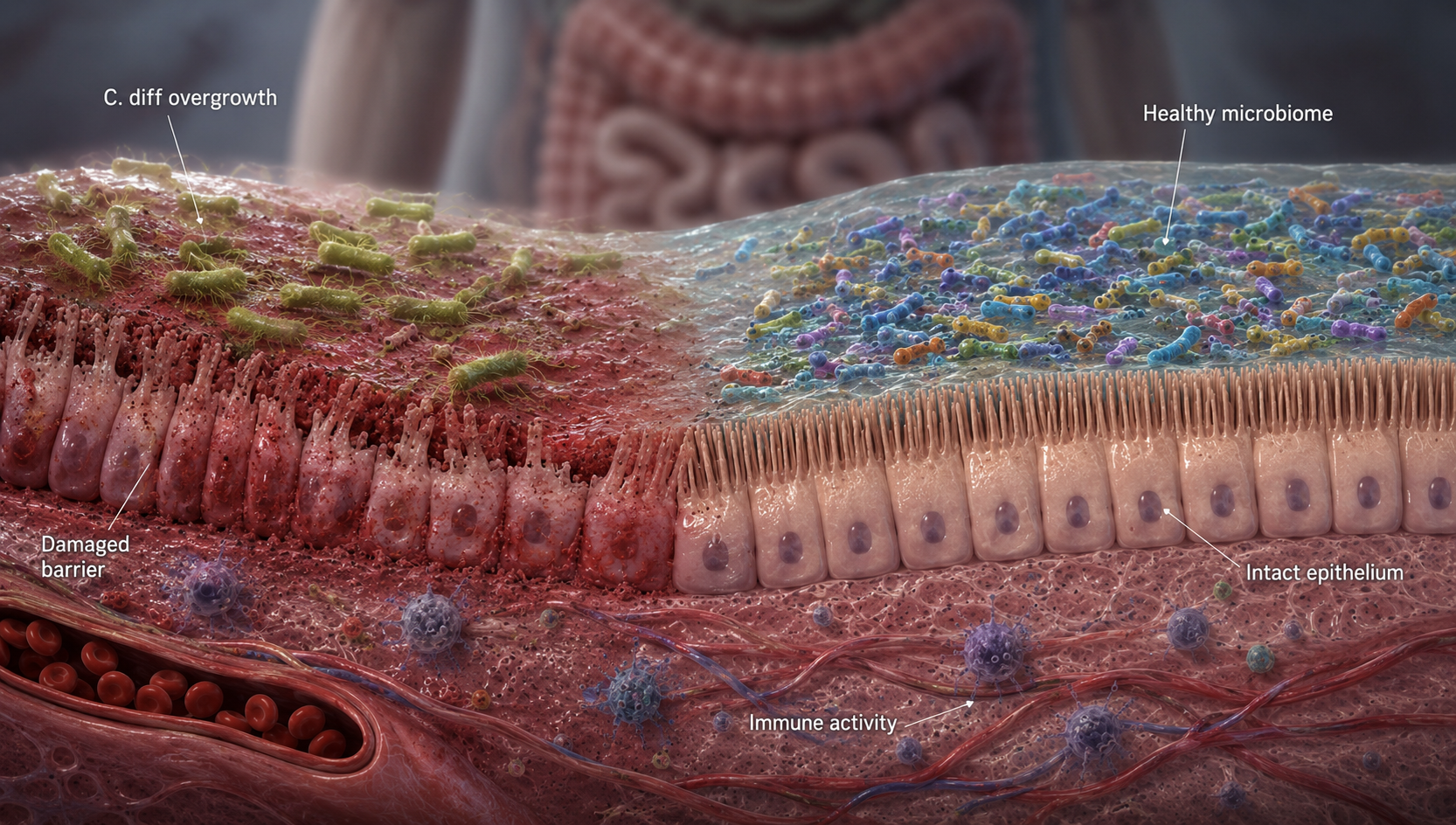
For patients with multiple recurrences, fecal microbiota transplantation (FMT) has emerged as a compelling option. By restoring a diverse gut microbiome, FMT addresses the ecological disruption that allows C. diff to re-establish — and the evidence base continues to grow.
The research consensus: early, proactive intervention, improved hospital surveillance, and whole-genome sequencing to track transmission chains are central to an evolving response to an infection whose full burden is still being measured.
Written by
MedBary Team
Comments
Log in to join the conversation.
Loading comments…