
Eyes Up: What Patients Think When AI Joins the Consultation
Every year, physicians lose thousands of hours to keyboards instead of patients. AI scribes are changing that — and patients have opinions.

The exam room is the most human space in medicine. Now an algorithm wants to listen. Every day, millions of clinical conversations vanish into keyboards — doctors typing while patients speak, a quiet friction that erodes the human core of care. AI scribes are changing that equation in real time, converting spoken words into clinical notes so physicians can look up. The question researchers are only beginning to answer is not whether the technology works, but whether patients genuinely want it — and what happens to trust, privacy, and the therapeutic relationship when an algorithm joins the room.

Physicians in the United States spend, on average, nearly two hours outside office hours each day keeping up with clinical notes. A landmark study tracking 57 doctors across multiple specialties found that physicians devoted only 27% of their working time to direct patient interaction, while nearly half was consumed by electronic health record tasks and desk work. This ratio is not merely inconvenient — it is a structural threat to care quality and to physician wellbeing.
Burnout among clinicians has reached near-endemic levels, with documentation burden cited consistently as a leading driver. Research published in the Journal of the American Medical Informatics Association found that over 46% of physicians felt they had insufficient time for documentation, and more than a third reported spending excessive hours on the EHR at home — a phenomenon researchers sometimes call "pajama time." The stakes extend beyond professional fatigue: when doctors are mentally occupied with keyboard logistics, patients feel it. Studies suggest that screen-focused behaviour in the exam room subtly diminishes the quality of non-verbal communication and erodes patient confidence in the encounter.
"A lot of people feel medical documentation is a necessary evil, but hate it when their doctors are sitting in front of the computer, trying to record everything they're talking about. They feel like that connection is lost."
— Dr. Gary Leiserowitz, Chair of Obstetrics and Gynecology, UC Davis Health
AI scribes enter this environment as a structural fix rather than a superficial convenience. By transcribing and summarising clinical encounters in real time, they free physicians to be genuinely present. The question of whether patients welcome that fix — and under what conditions — has real consequences for adoption rates, clinical trust, and the ethics of deploying AI in one of the most personal spaces in human life.

When UC Davis Health prepared to roll out an AI scribe program, its team took an unusual first step: they asked patients what they thought before deploying the technology. The resulting survey, published in JMIR Medical Informatics, reached more than 9,000 patients, of whom around 1,900 responded — and their answers revealed a population that was cautiously interested rather than categorically opposed.
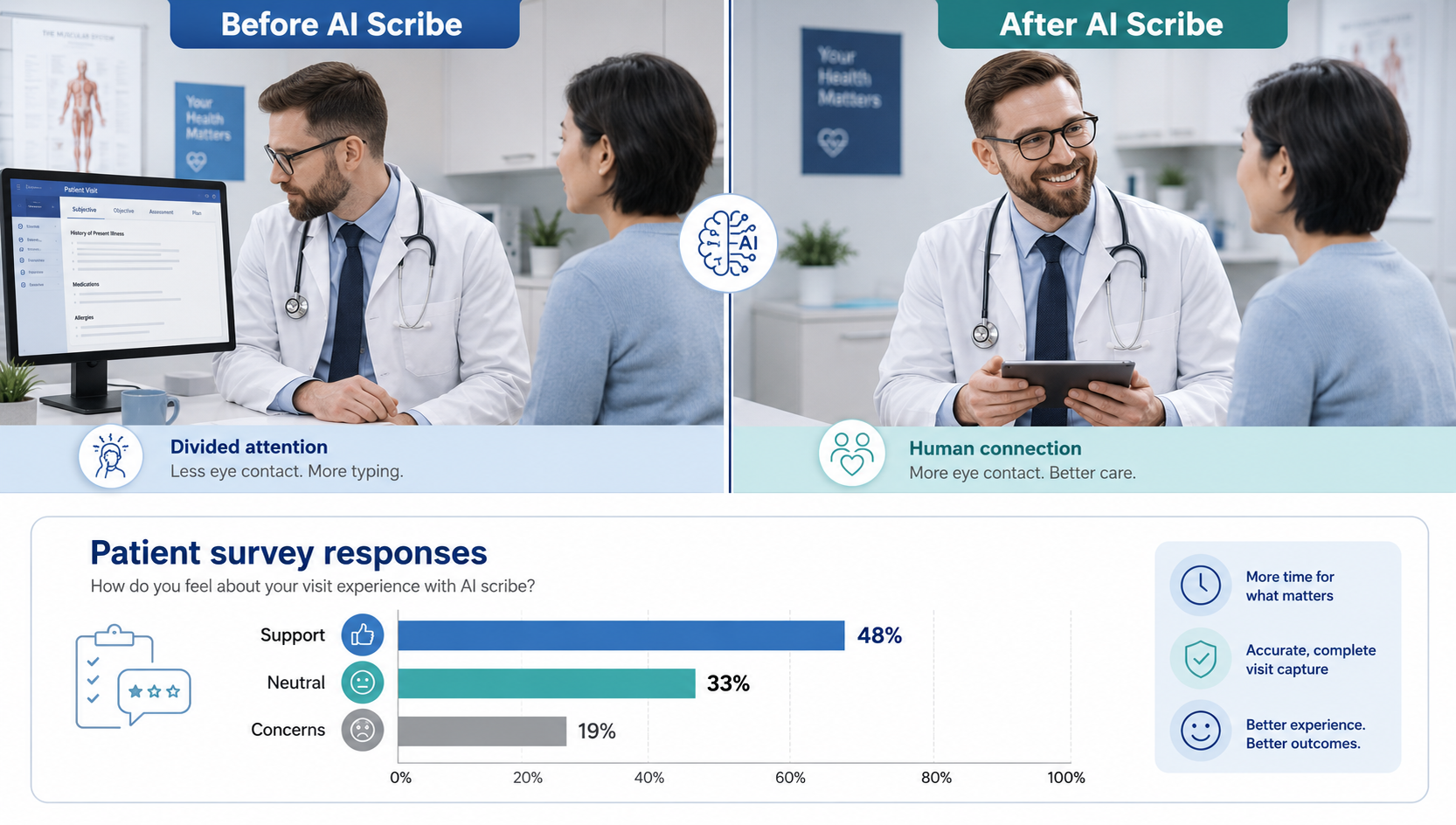
Nearly half of respondents — 48% — viewed AI scribes as a good solution to the documentation problem. A third were neutral. Around one in five had concerns, primarily centred on note accuracy, data privacy, and the prospect of being recorded. Notably, younger patients aged 18 to 30 expressed more scepticism than older cohorts — a finding that challenges the assumption that digitally native generations would be the most enthusiastic adopters. The explanation may lie in a heightened awareness of data surveillance among younger adults rather than any aversion to technology itself.
The survey also surfaced a critical practical insight: when patients are told about an AI scribe matters as much as how. Most strongly preferred to be informed early — at appointment booking, at clinic check-in, or upon arrival — rather than during or after the consultation. The majority favoured a face-to-face explanation over a digital notification. This points toward consent not as a procedural checkbox but as a relational act: patients want the conversation about AI to happen within the same trusted encounter where clinical care is offered.
Across a 63-week evaluation at The Permanente Medical Group — spanning 2.5 million encounters with 7,260 physicians — doctors using AI scribes saw significant reductions in after-hours note-writing and time per appointment. The top third of users saved two and a half times more time per note than lower-frequency adopters.
Forty-seven percent of patients reported their doctor spent less time looking at a screen. Thirty-nine percent said their physician spoke directly to them more. In dermatology trials, roughly three-quarters of patients described their appointment as feeling more like a genuine conversation after AI scribe introduction.
Psychiatry presents a more nuanced picture. A 2025 peer-reviewed analysis in Focus: Journal of Life Long Learning in Psychiatry (University of Pittsburgh) noted that while AI scribes show genuine promise for reducing clinician burnout and improving rapport, the psychiatric context demands particular caution. Patients experiencing paranoia or acute distress may have their therapeutic alliance threatened by a recording device. AI can also miss what researchers describe as "subtext" — the hesitations, tonal shifts, and nonverbal cues that often carry the clinical weight of a psychiatric interview. The recommendation is selective use: AI for capturing history and treatment plans, clinician-written notes for mental status examinations.
Privacy concerns thread through every patient perception study. At UC Davis, the implementation team responded directly to survey anxiety by committing to domestic-only data servers and a policy that audio recordings are deleted within ten days of the appointment. Clinicians review and edit every AI-generated note before it enters the permanent medical record — the AI produces a draft, not a final document. Patients also retain the right to opt out entirely.
One dimension of risk that has received less public attention is algorithmic bias. AI scribes are trained on large clinical datasets that inevitably reflect the demographic skews of the health systems that generated them. Patients from marginalised communities may find that AI-generated notes mischaracterise their symptom descriptions in subtle but clinically consequential ways. Physician review of every AI-generated note is not optional — it is the ethical and legal backstop on which responsible use depends.
The picture emerging from the evidence is neither a straightforward endorsement nor a cautionary rejection. Patients accept AI scribes when introduced transparently, when concerns about accuracy and privacy are addressed substantively, and when they can see the tool is returning their doctor's full attention to them. The technology is not a neutral background feature — it is a participant in the consultation, and patients respond to it accordingly.
| Source | Key Contribution | Published |
|---|---|---|
| UC Davis Health · JMIR Medical Informatics | Patient perception survey (n=1,900+); consent timing preferences; top concerns around accuracy, privacy & recording | Dec 2025 |
| The Permanente Medical Group · NEJM Catalyst | 63-week deployment; 7,260 physicians; 2.5M encounters; 1,794 working days saved; 84% physician satisfaction rate | Apr 2025 |
| Buckley, Wang & Gopalan · Focus (APA) PMC11701814 | Peer-reviewed review of AI scribes in psychiatry — risks, bias, hallucination, consent frameworks for mental health | Jan 2025 |
| Sinsky et al. · Annals of Internal Medicine | Time-motion study: 57 physicians; only 27% of clinic time on direct patient care vs 49% on EHR and desk tasks | 2016 |
| Gaffney et al. · JAMA Internal Medicine | National study: outpatient physicians averaged 1.8 hrs/day after-hours documentation; directly linked to burnout | 2022 |
All statistics and clinical findings cited are drawn exclusively from peer-reviewed publications and institutional health reports. No findings have been paraphrased in a manner that materially alters their original conclusions.
This article was produced for informational and journalistic purposes and draws exclusively on published, peer-reviewed research and institutional health reports. It does not constitute medical, legal, or technology procurement advice. The findings cited reflect the state of available evidence as of mid-2025 and early 2026 and are subject to revision as the field develops. Bloorian has no commercial relationship with any AI scribe vendor referenced or implied in this reporting.
Written by
MedBary Team
Comments
Log in to join the conversation.
Loading comments…