The path to LASSARAB began not in a single laboratory but through a convergence of immunological insights accumulated over more than a decade. Researchers studying survivors of severe Lassa infection observed a consistent pattern: those who recovered tended to mount an early, high-titer IgG antibody response directed at the viral glycoprotein complex (GPC) — the molecular structure the virus uses to attach to and enter human cells. Survivors also generated robust T-cell responses against both GPC and the viral nucleoprotein, all while keeping systemic inflammation comparatively low.
The challenge, however, was translating this observation into a vaccine candidate. Immune correlates of protection for Lassa remain incompletely understood — unlike some other pathogens, scientists cannot yet point to a single biomarker threshold and say definitively: above this level, a person is protected. Convalescent serum transferred from survivors to infected patients, once a promising therapeutic approach, failed to demonstrate consistent clinical benefit. Vaccine development has therefore required building on incomplete knowledge while simultaneously filling the gaps.
How LASSARAB Works
The Vector
An inactivated rabies virus serves as the delivery platform, carrying a Lassa glycoprotein antigen on its surface — a two-in-one immunological payload.
The Adjuvant
The TLR-4 agonist 3D-6acylPHAD-SE was paired with the vaccine to boost immune activation — a formulation strategy that amplifies the body's response without increasing reactogenicity.
The Cold Chain
LASSARAB can be freeze-dried, making refrigeration-independent storage possible — a defining practical advantage for distribution across rural West Africa where cold chains routinely fail.
The Phase 1 trial enrolled 54 healthy adults from the Baltimore area who were randomized to receive either two intramuscular doses of LASSARAB — at antigen concentrations of 700, 1,400, or 2,800 relative units — or a licensed rabies vaccine as a control. Doses were given 28 days apart. After both doses, every participant in all three LASSARAB dose groups achieved more than a fourfold increase in IgG antibodies against the Lassa glycoprotein complex, as measured by ELISA. The same recipients also showed the same magnitude of rabies antibody response. The control group, receiving only licensed rabies vaccine, demonstrated rabies-only immune response, as expected.
Adverse events across all groups were reported as predominantly mild and self-limiting — the kind of post-vaccination soreness and transient fatigue that characterizes most vaccine trials at this stage. No serious adverse events were recorded through Day 61, the interim reporting point. The study will continue monitoring participants for 394 days, evaluating both the durability of immune responses and long-term safety — data that will be essential for advancing to Phase 2 trials.
The platform itself — using the rabies virus as a vector — deserves particular attention from a public health strategy standpoint. Rabies kills an estimated 59,000 people annually worldwide, with the overwhelming burden concentrated in Africa and Asia. In the very communities where Lassa fever circulates most intensely, rabies exposure from dog and bat bites is a persistent threat. A vaccine that simultaneously confers protection against both pathogens does not simply double the benefit; it changes the economics and logistics of immunization programs in resource-limited settings. Fewer vaccination campaigns, fewer doses to procure and cold-store, fewer healthcare worker visits required — all meaningful reductions in a setting where each of those factors constrains how many people can actually be reached.
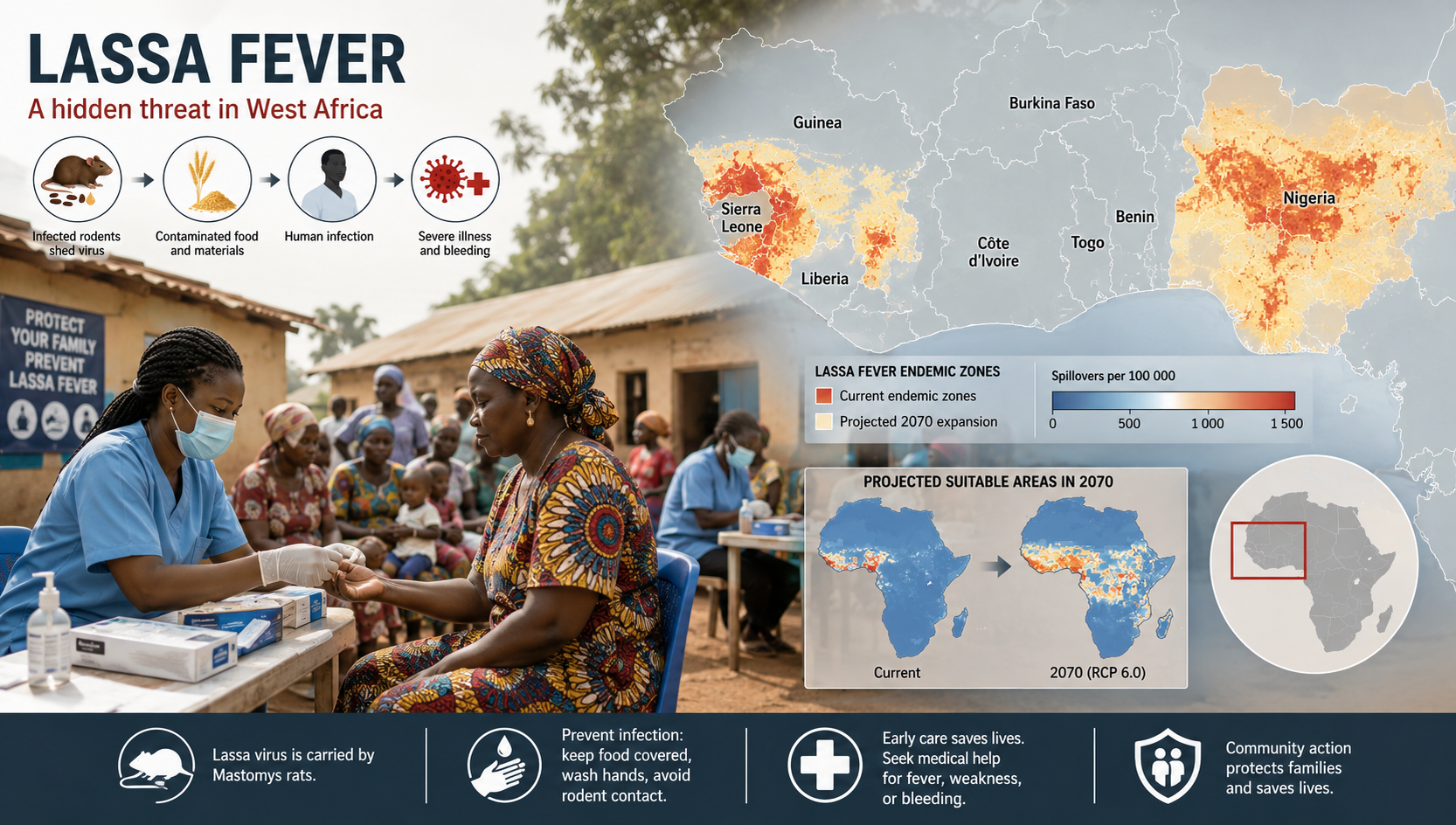
The groundwork for this moment was laid across multiple institutions over many years. At Tulane University, immunologist Robert Garry and his colleagues spent more than a decade mapping how the Lassa glycoprotein complex presents itself to antibodies, identifying which molecular surfaces are most accessible to neutralizing immune responses. Tulane researchers discovered that the virus had existed in Nigeria for roughly a thousand years and in Sierra Leone for around 150, tracing its genetic evolution across four distinct strains. That strain diversity is one reason a broadly effective vaccine has been so difficult to achieve — the target has been moving.
James Robinson, Garry's colleague at Tulane, developed methods to isolate Lassa-specific antibodies from survivor blood samples — screening thousands of B-cell cultures, one color change at a time, to find those rare cells carrying antibodies capable of neutralizing the virus in the lab. That tedious, careful work identified the antibody targets that the LASSARAB vaccine's design would eventually seek to stimulate. The Thomas Jefferson University team, led by Matthias Schnell, then engineered the inactivated rabies vector to display those Lassa antigens on its surface — the technical bridge between survivor immunology and an injectable product.
The first-in-human result does not mark the end of this journey. It marks the moment the scientific hypothesis moved from animal models to verified human biology. What follows will require Phase 2 trials with larger and geographically diverse populations — including, ultimately, participants within Lassa-endemic communities themselves. Regulatory review, manufacturing scale-up, and delivery infrastructure will each present their own obstacles. But for a disease the World Health Organization has prioritized as a global health threat without an approved vaccine, the Phase 1 data from June 2026 represents one of the most consequential early results in infectious disease research this decade.