
Hospital Strategic Planning: A Step-by-Step Framework
Hospital strategic planning is not a document prepared every few years. It is a leadership system for choosing priorities, aligning resources, measuring execution, and adapting when the market, workforce, or patient needs change. The strongest plans connect clinical quality, financial sustainability, community need, access, workforce capacity, and governance into one accountable operating model.


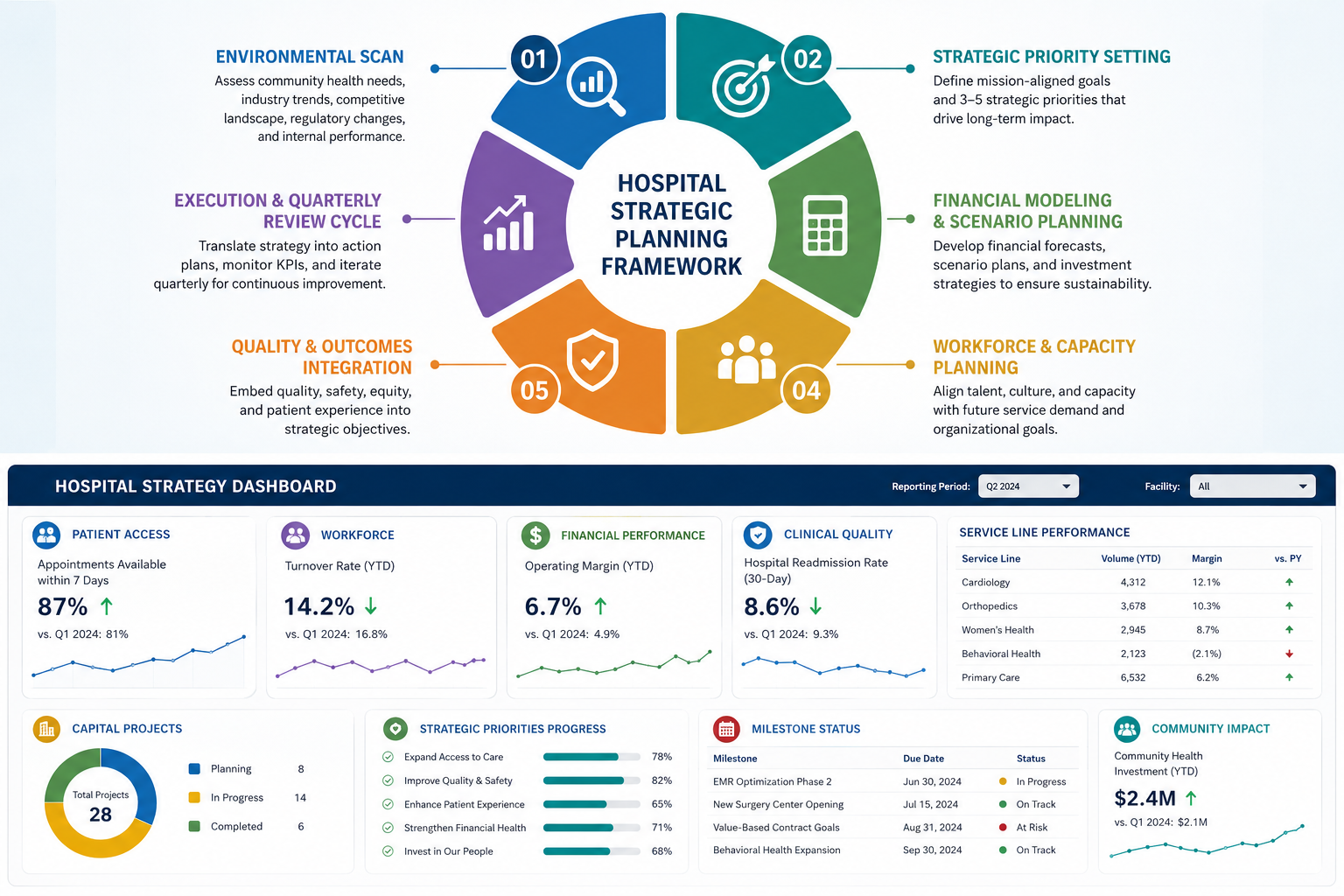
Six disciplines that turn a hospital plan into a working strategy
Start with the real environment
Build the plan around demand, population health, referral patterns, payer mix, workforce pressure, access barriers, financial capacity, and local competition.
Choose fewer priorities
A plan with too many major priorities becomes a wish list. Most organizations need three to five measurable enterprise commitments.
Connect strategy to money
Each priority needs a financial model, investment estimate, accountable owner, timeline, risk assessment, and measurable value outcome.
Plan for workforce capacity
Service-line growth, access expansion, quality improvement, and digital transformation depend on people, skills, workflow, and leadership capacity.
Use quality as a strategic measure
Patient safety, equity, access, experience, and clinical outcomes should sit inside the enterprise plan rather than beside it.
Review and adapt continuously
Strategy needs quarterly review, transparent dashboards, clear accountability, and timely course correction when conditions change.
Hospitals cannot solve interconnected problems through disconnected planning.
Hospital leaders are expected to manage workforce shortages, changing patient expectations, rising operating costs, payer pressure, outpatient migration, new technologies, cyber risk, quality requirements, and growing access needs at the same time. When these issues are treated as separate projects, the result is often fragmented budgets, competing priorities, and exhausted leadership teams.
Strategic planning creates a shared decision framework. It helps the board, executive team, clinical leaders, and operational departments agree on what the organization will prioritize, what it will defer, where it will invest, and how progress will be judged. This matters because resources are limited, but the consequences of poor choices can affect patient access, staff retention, community trust, and financial resilience.
National health spending in the United States reached $5.3 trillion in 2024, or 18 percent of gross domestic product, illustrating the scale and complexity of the environment in which hospitals operate.[1] A strategic plan cannot remove uncertainty, but it can help an organization respond to uncertainty with discipline rather than reaction.
A practical framework for building a hospital strategy that survives contact with reality
Most hospital strategic plans do not fail because leaders lack ambition. They fail because the plan is designed as a publication rather than an operating system. A leadership retreat produces a vision statement, a consultant develops a market report, the board approves a list of priorities, and the organization announces a new direction. Then daily operational pressure returns. Staffing gaps, delayed discharges, revenue-cycle concerns, patient complaints, capital requests, physician recruitment, and compliance demands take over. Without an execution structure, the strategy gradually becomes a document stored in a shared drive.
A stronger approach starts with a different premise: strategy is a continuous management discipline. It is the process through which leaders choose where the hospital should compete, what services should grow, which risks require investment, what performance should improve, and what must stop or change. The written plan matters, but it is only one output. The real outcome is alignment across the organization.
1. Begin with an honest environmental scan
Strategic planning should begin with evidence, not internal assumptions. A hospital needs a clear view of its current market position before it decides where to go. This means studying population growth, age distribution, disease burden, referral leakage, appointment wait times, payer mix, service-line demand, physician availability, workforce turnover, competitor expansion, and community access barriers.
Internal performance matters equally. Leaders should review operating margin, cash position, revenue cycle performance, quality outcomes, length of stay, readmissions, workforce vacancy rates, patient experience, technology debt, capital condition, and service-line contribution. The objective is not to collect every possible metric. It is to identify the trends that create strategic consequences.
For example, a growing older adult population may signal a need to strengthen cardiology, orthopedics, rehabilitation, chronic disease care, home-based services, and transitional care. A shift from inpatient to outpatient utilization may require investment in ambulatory care, digital scheduling, imaging, urgent care, telehealth, and better referral management. Strategy becomes credible when it responds to observed need rather than internal habit.
2. Turn information into clear strategic choices
Strategy is fundamentally about choice. A hospital cannot lead in every specialty, serve every geography equally, or invest in every technology at once. Leadership teams must determine where the organization can create the greatest clinical, financial, and community value. This often requires difficult discussions about which programs should expand, which should stabilize, and which may no longer fit the organization’s long-term direction.
Effective priorities are specific enough to guide action. “Improve patient experience” is an important aspiration but not a complete strategic commitment. “Reduce first-available specialty appointment waits by 30 percent in cardiology, orthopedics, and oncology while improving patient communication scores” provides an outcome, a scope, and a measurable target.
Most hospitals benefit from limiting enterprise priorities to three to five. These may include financial sustainability, access expansion, workforce resilience, digital modernization, quality improvement, targeted service-line growth, or community partnership. Every department does not require its own enterprise strategy. Instead, departmental goals should support the few priorities chosen by the organization.
3. Build a financial and operational case for every priority
A strategic priority without a financial model is a wish. Every major initiative should identify the capital requirement, annual operating cost, workforce requirement, technology dependency, expected revenue effect, quality effect, risk profile, and implementation timeline. Not every investment must produce immediate profit. Some investments protect access, improve safety, reduce future risk, or preserve workforce capacity. However, leaders should still understand the cost, the rationale, and the expected value.
Financial modeling should include several scenarios. What happens if volume grows more slowly than expected? What happens if hiring takes longer than planned? What happens if reimbursement changes? What happens if the project requires more capital or takes an additional year to implement? Scenario planning makes assumptions visible before an organization commits scarce resources.
Capital planning should also follow strategy. A new operating room, outpatient site, imaging platform, specialty clinic, scheduling system, or digital patient-access tool should exist because it supports a defined strategic choice. Capital projects become risky when they are driven mainly by historical practice, individual preference, or fear of competitor activity without a clear demand and value analysis.
4. Treat workforce capacity as a strategic constraint
Workforce planning is no longer a supporting function beside hospital strategy. It is one of the central limits on what organizations can deliver. A service-line growth plan cannot succeed without enough physicians, nurses, technologists, therapists, administrative staff, schedulers, revenue-cycle professionals, and operational leaders to support it.
Workforce analysis should go beyond vacancy counts. Hospitals need to understand turnover hotspots, burnout risk, compensation pressure, productivity patterns, leadership succession, internal mobility, clinical education needs, and the roles that could be redesigned through technology or team-based care. New services may require new skills, revised workflows, different staffing ratios, or stronger partnerships with academic and community organizations.
HRSA’s performance-improvement tools specifically connect workforce, financial sustainability, quality, access, patient experience, governance, and strategic planning.[2] The practical lesson is clear: a strategic plan that ignores workforce realities is not a strategy. It is an aspiration without a delivery model.
5. Place quality, safety, and patient experience inside the business strategy
Quality, patient safety, equity, access, and experience should not sit outside the business plan as separate clinical initiatives. Poor quality creates direct operational consequences through rework, preventable cost, staff frustration, lost trust, reduced referrals, regulatory exposure, and reputational damage. Strong quality performance can support both patient outcomes and organizational sustainability.
AHRQ describes quality improvement as a systematic approach to analyzing performance and improving care processes.[3] Hospital strategy should use the same discipline. Leaders need clear measures, transparent reporting, frontline participation, patient feedback, and structured improvement cycles. A strategy that cannot be measured cannot be managed.
Patient and community perspectives should also shape the planning process. Advisory councils, listening sessions, complaint-theme analysis, access data, survey feedback, and community health assessments can reveal problems that traditional executive dashboards do not capture. Patient-centered planning is not only about satisfaction. It is about designing services around the actual experience of receiving care.
6. Create a governance and execution rhythm
Execution is where strategy becomes real. Each priority should have an executive sponsor, operational owner, measurable outcomes, budget, milestone plan, risk register, and regular review process. At any moment, leaders should be able to answer five questions: What are we trying to achieve? Who owns the work? What progress has been made? What is blocking progress? What decision is needed next?
Board involvement is essential, but it should remain governance-focused. The American Hospital Association notes that boards should be meaningfully involved in shaping and approving strategic direction while management develops and executes the operational plan.[4] Clear roles prevent the board from becoming an operating committee and prevent management from treating the board as a passive audience.
A practical strategy dashboard should use both leading and lagging indicators. Leading indicators may include recruitment progress, new-patient access, project milestones, referral conversion, patient portal adoption, training completion, or partnership development. Lagging indicators may include operating margin, quality outcomes, market share, patient experience, turnover, readmissions, and cost per case. Quarterly review helps leaders adapt before small problems become structural failures.
Sources used for context
Editorial Note: This article is produced for informational and educational purposes. It does not constitute medical advice. Patients should consult a qualified healthcare provider for diagnosis and treatment guidance. All statistics cited are sourced from peer-reviewed literature or named patient advocacy organizations as referenced above.
Written by
MD Zee
Comments
Log in to join the conversation.
Loading comments…