

ICU Management: Balancing Quality Care with Cost Efficiency
Intensive care units are the highest-cost, highest-revenue, and highest-risk environment in any hospital. This article breaks down the financial levers, staffing models, and operational strategies that separate elite ICUs from expensive ones.


The intensive care unit is the highest-acuity, highest-cost, and highest-stakes environment in any hospital. A single ICU bed costs a health system an estimated $3,500 to $5,000 per day to operate — roughly four to five times the cost of a standard medical-surgical bed. Patients who occupy those beds are among the most clinically complex in the facility, requiring round-the-clock specialist oversight, advanced monitoring technology, and nurse-to-patient ratios that no other department demands. For hospital executives and healthcare business consultants, the ICU represents both the greatest concentration of clinical risk and one of the most significant levers for operational and financial improvement in the entire hospital.
The Financial Reality of Critical Care
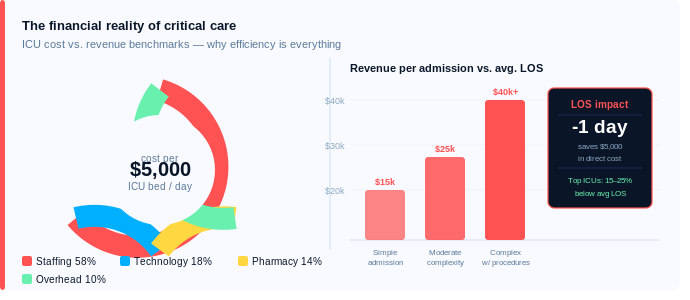
Critical care is simultaneously one of the highest-revenue and highest-cost service lines in hospital medicine. Medicare and commercial insurers reimburse ICU care at premium rates — a complex critical care visit with procedures can generate $15,000 to $40,000 or more in revenue for a single admission. Yet those revenues are frequently eroded by inefficiencies that are entirely within a hospital's control.
Length of stay is the single most important financial variable in the ICU. Every additional day a patient spends in an intensive care bed that could be managed on a step-down or medical-surgical floor represents both unnecessary cost and a bed unavailability problem for the next critically ill patient. Benchmark ICU length of stay varies by diagnosis and case mix, but high-performing units consistently achieve lengths of stay 15 to 25 percent below national averages through structured daily goal-setting, multidisciplinary rounds, and aggressive discharge planning to step-down units.
Staffing costs are the other dominant financial driver. ICU nursing requires advanced certification and commands premium compensation — typically 20 to 35 percent above standard nursing rates. Intensivist physician coverage — whether through employed hospitalists, pulmonary critical care specialists, or telemedicine-based tele-ICU programs — adds another significant layer of cost that must be justified by measurable outcomes improvements and length of stay reductions.
The financial case for investing in ICU excellence is compelling. Hospitals with high-performing ICUs consistently report lower mortality rates, fewer hospital-acquired complications, shorter lengths of stay, and higher patient and family satisfaction scores — all of which translate directly into better reimbursement, reduced penalty exposure under value-based purchasing programs, and stronger competitive positioning.
Staffing Models and the Tele-ICU Revolution
The question of how to staff an ICU is one of the most consequential operational decisions a hospital can make. Research consistently demonstrates that closed ICU models — in which a dedicated intensivist team controls all patient care decisions — produce superior clinical outcomes compared to open models where any admitting physician can manage ICU patients. Closed models reduce mortality, decrease length of stay, lower complication rates, and improve nursing satisfaction. Yet many community hospitals struggle to implement them due to the limited supply of board-certified intensivists and the political complexity of restructuring physician admitting privileges.
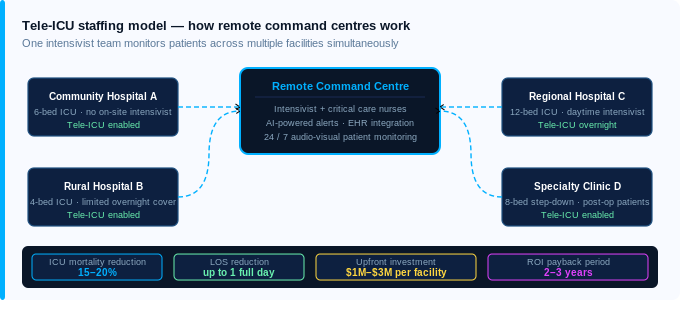
Tele-ICU technology has emerged as a powerful solution to this staffing challenge, particularly for rural and community hospitals that cannot recruit or retain full-time intensivists. In a tele-ICU model, a remotely located team of intensivists and critical care nurses monitors ICU patients across multiple facilities in real time using audio-visual technology, electronic health record integration, and AI-powered alert systems. Studies have shown that tele-ICU programs reduce ICU mortality by 15 to 20 percent and lower length of stay by up to a full day — representing both significant clinical benefit and meaningful cost reduction.
From a business perspective, tele-ICU programs require meaningful upfront investment in technology infrastructure — typically $1 million to $3 million for a mid-sized community hospital — but the return on investment through reduced length of stay, avoided complications, and the ability to treat higher-acuity patients locally rather than transferring them to tertiary centers is well documented and frequently exceeds the investment within two to three years.
Operational Excellence in the ICU
Beyond staffing models, several operational practices consistently differentiate high-performing ICUs from average ones. Structured multidisciplinary rounds — conducted daily with intensivists, nurses, pharmacists, respiratory therapists, and case managers — are the single most evidence-based intervention for improving ICU efficiency. These rounds establish daily goals for each patient, identify barriers to discharge, and ensure that every member of the care team is aligned on the clinical plan and the timeline.
Bundles of care — standardized protocols for preventing ventilator-associated pneumonia, central line infections, pressure injuries, and venous thromboembolism — are non-negotiable in high-performing ICUs. Beyond their obvious clinical benefit, these bundles have direct financial implications. Hospital-acquired conditions in the ICU are not reimbursed by Medicare and trigger financial penalties under the Hospital-Acquired Condition Reduction Program. Every preventable complication is both a patient harm and a revenue loss.
Family communication and engagement is an often-overlooked operational lever. ICU families who are well-informed, involved in care planning, and supported through the emotional complexity of critical illness make faster and better-informed decisions about goals of care — including appropriate transitions to palliative or comfort care when curative treatment is no longer beneficial. This reduces unnecessary ICU utilization at end of life, which is both ethically appropriate and financially significant.
Key Takeaway
The ICU is too important — clinically and financially — to manage by intuition alone. Health systems that approach critical care with the same analytical rigor they apply to their highest-revenue service lines consistently outperform those that treat the ICU as simply a clinical necessity. The investment in intensivist coverage, tele-ICU technology, structured rounding protocols, and care bundles pays dividends in outcomes, efficiency, and financial performance.
Is your ICU operating at its clinical and financial potential? A focused critical care operational assessment can identify the staffing model, technology investments, and process improvements that will drive measurable gains in quality, efficiency, and margin within 90 days.
Written by
MD Zee
Comments
Log in to join the conversation.
Loading comments…