
Mantle Cell Lymphoma Is Changing Its Face. Health Systems Aren't Keeping Up.
The incidence numbers are moving. The patient profile is shifting. And the cascade of therapies MCL demands — BTK inhibitors, stem cell transplant, CAR-T — means every additional case carries an outsized price tag.

Mantle cell lymphoma has long been framed as a disease of older men — an aggressive, rare blood cancer with limited options and a predictably grim arc. But national surveillance data now tell a different story. Women are being diagnosed at accelerating rates. Younger adults are entering treatment pathways once reserved for the elderly. And the cumulative pressure on health systems, payers, and research priorities is building in ways the field is only beginning to quantify.
Key Highlights
What the data are showing
Projected rise in MCL among women by 2032
From roughly 920 to 1,318 new cases per year — a demographic shift that directly challenges the disease's longstanding profile as a condition of older men.
Rise in diagnoses among patients under 65
MCL is no longer an elderly-only disease. Younger diagnoses mean decades of treatment ahead — compounded lifetime costs that commercial insurers, not just Medicare, will bear.
Overall MCL incidence growth through 2032
From 3,377 to 3,589 new annual cases. Modest in count — but MCL's resource-intensive multi-line cascade amplifies every additional case into significant systemic cost.
Reach first-line systemic therapy
Nearly half then advance to a second line — and nearly half of those to a third. The cycle runs through BTK inhibitors, immunochemotherapy, stem cell transplant, and CAR-T therapy.
% OF PRIOR-LINE PATIENTS ADVANCING · SEER-MEDICARE 2012–2021
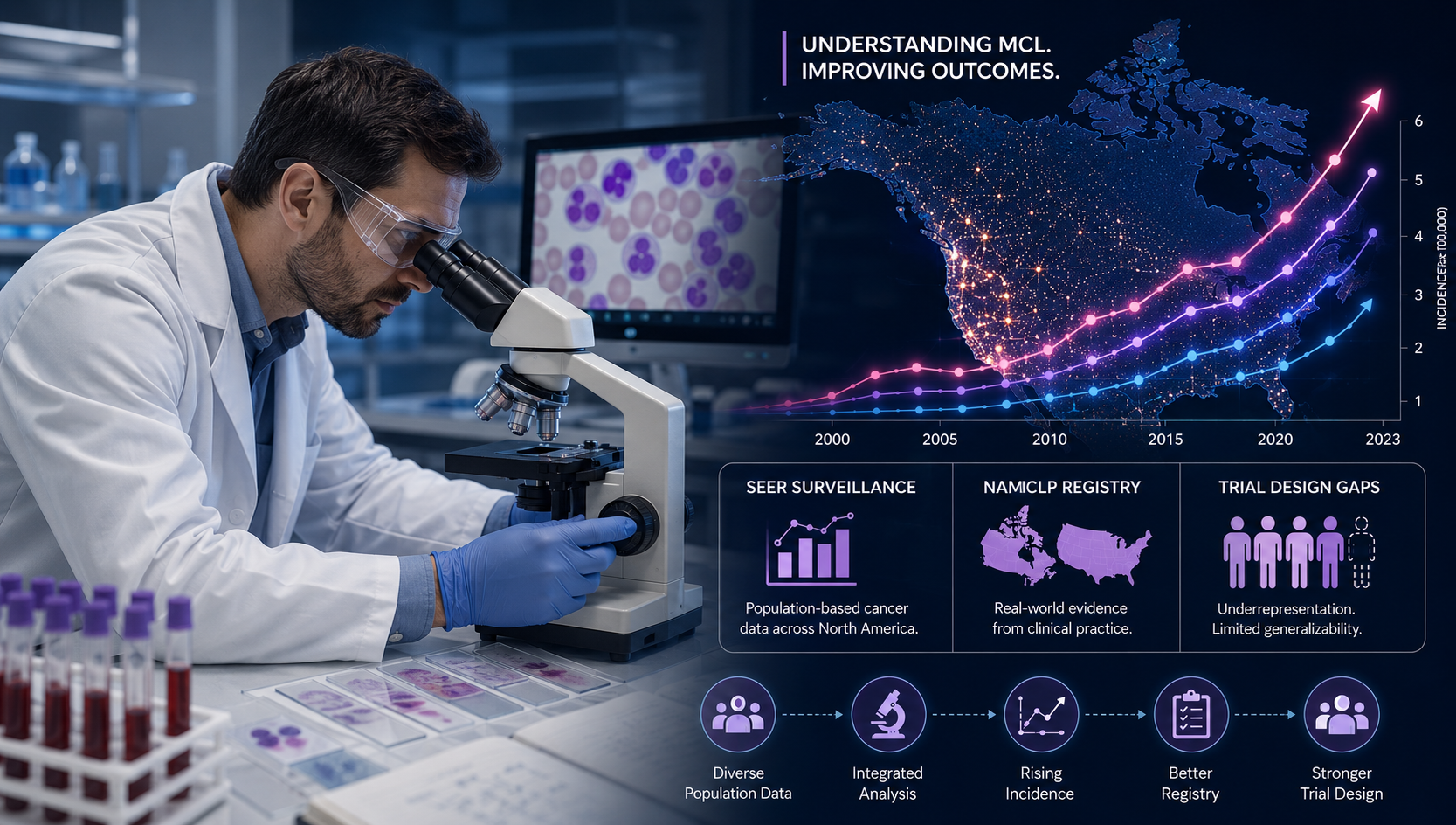
Mantle cell lymphoma sits in an uncomfortable category within hematological oncology — too rare to attract the research investment more common cancers command, yet clinically aggressive enough to demand the most resource-intensive treatment protocols available. It makes up roughly 6% of all non-Hodgkin lymphoma diagnoses. Historically a disease of older men, it typically presents at an already-advanced stage with widespread lymph node involvement, bone marrow infiltration, and frequent spread to the gastrointestinal tract.
That profile is shifting. Population-level data drawn from the National Cancer Institute's SEER surveillance program — spanning over a decade of incidence records and Medicare claims — document trends oncologists cannot attribute to changes in diagnostic sensitivity alone. A 43% projected rise in MCL diagnoses among women, and a 33% increase among patients under 65, reflect a genuine epidemiological evolution unfolding in real time.
of MCL patients receive first-line systemic therapy — with nearly half then progressing through second, third, and fourth lines of increasingly costly treatment.
For the healthcare system, this demographic shift carries weight on multiple fronts. Younger patients are less likely to be Medicare-enrolled, redirecting financial pressure toward commercial insurers and employer benefit plans — entities far less equipped to absorb the costs of a multi-line hematological cancer. Women with MCL have been historically underrepresented in clinical trials, raising real questions about whether current protocols are optimally designed for this growing cohort.
The treatment cascade for MCL — spanning induction immunochemotherapy, autologous stem cell transplantation, second-generation BTK inhibitors, and CAR-T cell therapy — is among the most resource-intensive in hematology. When a growing number of patients enters this cascade earlier in life, the cumulative lifetime burden per patient expands in ways no projection model yet fully captures.

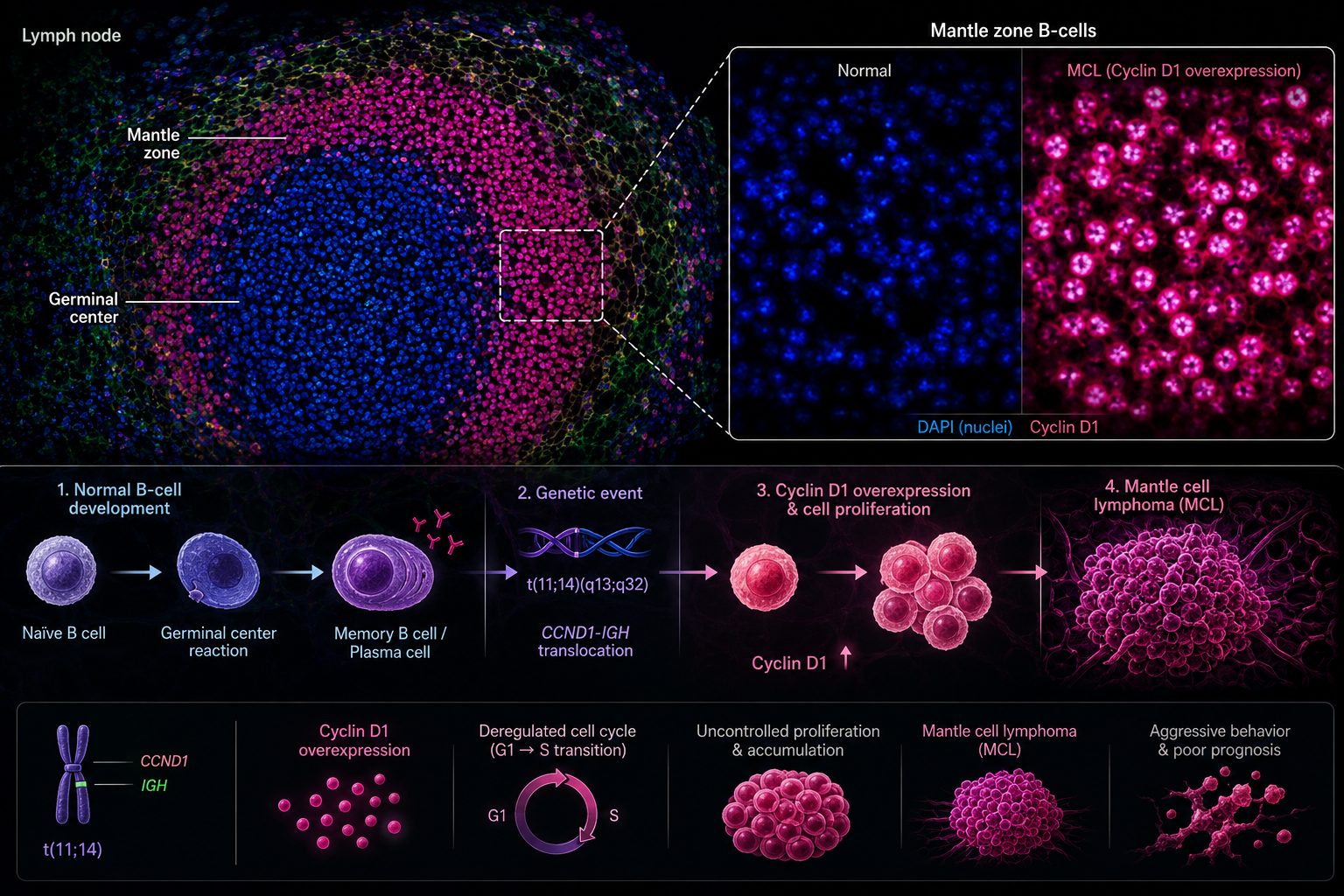
The biology of MCL begins at the chromosomal level. A translocation between chromosomes 11 and 14 — t(11;14) — leads to overexpression of cyclin D1, driving B-lymphocytes in the mantle zone of lymph follicles to multiply without restraint. Unlike some lymphomas that permit a period of watchful waiting, most MCL presentations demand prompt, aggressive intervention. The disease frequently arrives at diagnosis already widespread, complicating both staging and treatment selection.
"The convergence of a rising female patient population, younger diagnoses, and an increasingly complex treatment armamentarium is reshaping what MCL care looks like — and who is ultimately paying for it."
The North American Mantle Cell Lymphoma Project (NAMCLP), based at the University of Nebraska Medical Center, is one of the most comprehensive ongoing efforts to characterize MCL across real-world North American populations. As the patient population becomes more demographically diverse, sex-stratified and age-stratified data become foundational — not supplementary — to guiding treatment guidelines.
More women
with MCL by 2032
Rise in diagnoses
under age 65
Reach first-line
systemic therapy
On the treatment frontier, an international Phase 3 randomized trial co-authored by investigators at the Ottawa Hospital Research Institute and published in The Lancet demonstrated that second-generation BTK inhibitors can significantly extend survival in relapsed or refractory MCL. Agents including acalabrutinib and zanubrutinib offer improved tolerability profiles — particularly significant for younger patients and women who may experience cardiac side effects at different rates than the older male populations that historically dominated trial enrollment.
CAR-T cell therapy has emerged as a critical salvage option for multiply relapsed MCL. Brexucabtagene autoleucel achieved regulatory approval on durable complete responses in heavily pre-treated patients, with some trials reporting complete response rates exceeding 50%. The challenge is access: CAR-T requires specialized manufacturing, certified treatment centers, and costs reaching hundreds of thousands of dollars per patient. As more women and younger patients eventually reach CAR-T eligibility, that economic pressure compounds substantially.
Secondary central nervous system involvement in MCL carries a devastating prognosis when it occurs. A 2025 analysis identified measurable risk factors for CNS progression — reinforcing the need for comprehensive staging and continuous monitoring. For younger patients, CNS relapse is particularly consequential: their longer life expectancy means more years navigating a condition for which effective salvage options remain scarce.
The Lymphoma Research Foundation's MCL Scientific Meetings have increasingly highlighted the need for clinical trials whose populations more accurately mirror the real-world disease distribution — including women, patients under 65, and individuals with comorbidity profiles historically excluded from enrollment. Designing the next generation of MCL trials with representativeness as a foundational requirement is no longer optional — it is overdue.
References
Citations & Source Credibility
Peer-reviewed journals · federal registries · academic institutions
Lin D, Shao C, Ma J, Burcu M, Sineshaw HM. Projected disease burden and treatment eligibility of patients with diffuse large B-cell and mantle cell lymphoma in the United States over the next decade. Cancer Treatment and Research Communications. 2026;48:101291.
North American Mantle Cell Lymphoma Project (NAMCLP). University of Nebraska Medical Center, Division of Oncology & Hematology. unmc.edu/intmed/divisions/onchem/research/namclp.html
Lymphoma Research Foundation. MCL Scientific Meetings. lymphoma.org/researchers/scientificmeetings/mclscientificmeetings/
Cancer Research UK. Mantle Cell Lymphoma. cancerresearchuk.org/about-cancer/non-hodgkin-lymphoma/types/mantle-cell
Ottawa Hospital Research Institute. When cancer comes back: drug for mantle-cell lymphoma gives patients more time. ohri.ca/en/newsroom/when-cancer-comes-back-drug-mantle-cell-lymphoma-gives-patients-more-time
Trab et al. Secondary CNS lymphoma (SCNSL) in mantle cell lymphoma (MCL). 2025. Aalborg University VBN Research Repository. vbn.aau.dk
NCI SEER Program. SEER-21 Incidence Data 2017–2022 and SEER-Medicare Claims 2012–2021. National Cancer Institute. seer.cancer.gov
University of Virginia Health. UVA co-hosts International Mantle Cell Lymphoma Research Symposium. news.med.virginia.edu
Institutional references do not imply editorial endorsement.
Topics
Editorial Note
This article is intended for informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment guidance. Projections cited are modeled estimates derived from federal surveillance data and are subject to revision as new evidence emerges. Readers are encouraged to consult qualified healthcare professionals for all clinical decisions. No commercial relationships influenced the preparation or editorial direction of this content.
Written by
MedBary Team
Comments
Log in to join the conversation.
Loading comments…