
The Bargain We Make With the Sun
For generations, we've bargained with the sun in silence, and paid the price in ways we're only beginning to understand. Dermatology is rewriting the terms.

Every summer, millions of people make a quiet bargain with the sun — some protection, some exposure, hope for the best. But decades of research are making it harder to justify that gamble. From immunotherapy breakthroughs reversing late-stage melanoma to a first new FDA-accepted sunscreen ingredient in twenty years, dermatology is rewriting what sun safety looks like at every level — cellular, clinical, and cultural.
This article examines the latest science on UV radiation, sunscreen efficacy, skin cancer immunology, and what clinicians and patients alike need to know heading into the peak sun months.

Between one million and five million new cases of basal and squamous cell carcinoma are diagnosed in the United States each year — numbers so large they aren't even formally tracked by cancer registries. Melanoma, though rarer, is responsible for an estimated 75 to 80 percent of all skin cancer deaths. In 2020, roughly 100,000 new melanoma diagnoses were recorded, alongside nearly 7,000 deaths.
Yet the disease is not evenly distributed. Racial disparities in melanoma survival remain stark: while the five-year survival rate among white patients approaches 94%, it sits at roughly 70% among Black patients — in part because acral melanomas affecting non-sun-exposed areas are caught later and less reliably recognised by clinicians trained on a narrower range of presentations.
Meanwhile, two converging forces are making the stakes higher. First, ozone layer thinning has increased the volume of cancer-spawning UV radiation reaching Earth's surface — the WHO projects a 10% rise in skin cancer among U.S. populations of European descent by 2050. Second, a warming climate amplifies this damage: one study found that UV radiation becomes roughly 5% more carcinogenic for every 1°C rise in environmental temperature.
"Science has melanoma on the run. But it hasn't eradicated the disease in any way." — Hensin Tsao, MD, HMS Professor of Dermatology, Massachusetts General Hospital

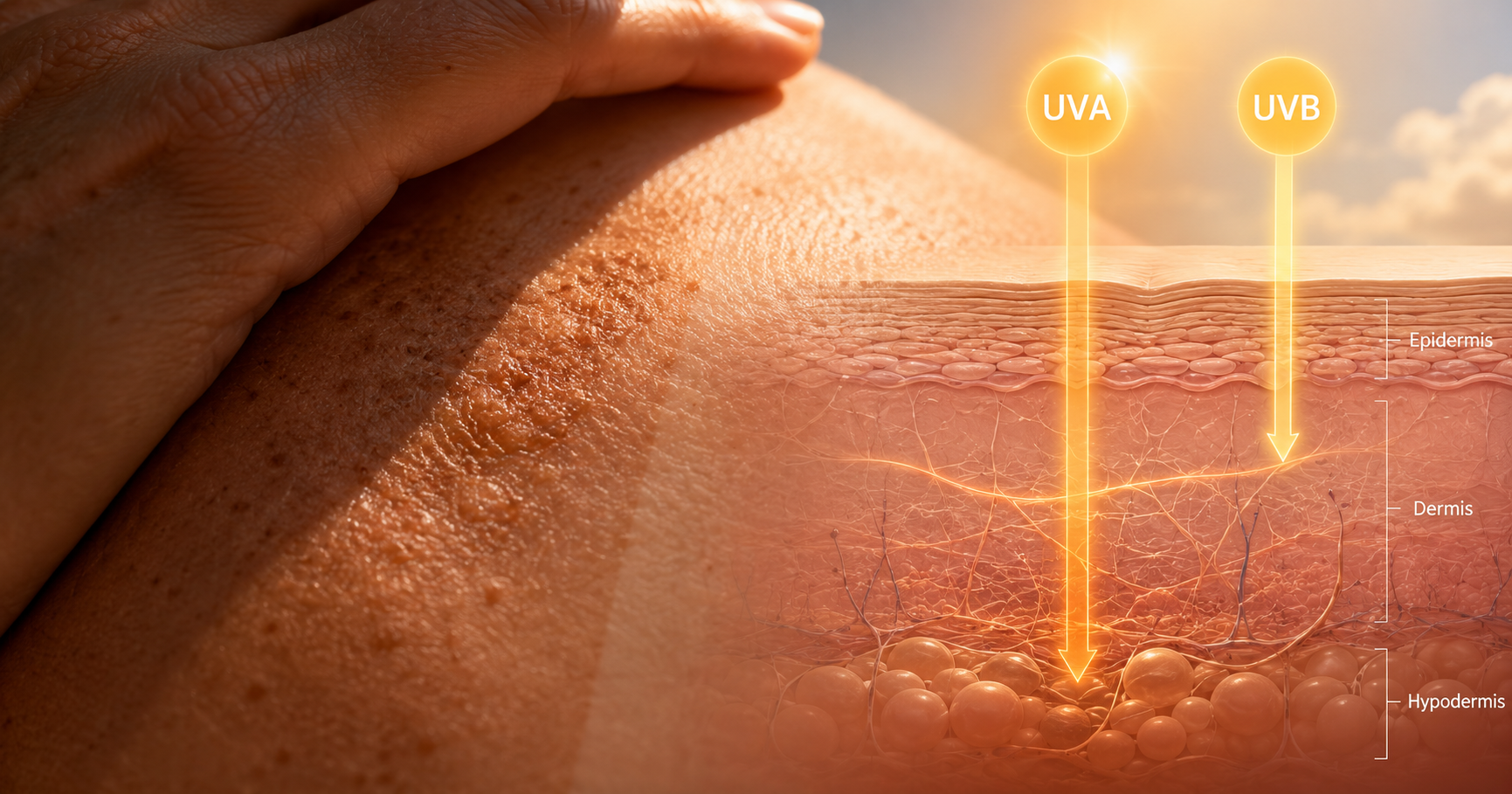
Ultraviolet radiation arrives in two clinically relevant forms. UVB rays — shorter in wavelength — cause direct DNA damage capable of triggering the mutations that seed skin cancer. UVA rays penetrate deeper, generating oxidative stress and inflammation that accelerates photoageing and contributes to carcinogenesis. "Most people know that sunscreen can help prevent sun-related skin cancer," said Stanford dermatologist Zakia Rahman, MD, "but they don't know the impact on photo-ageing. A lot of people want their skin to look better, and UV light really accelerates premature aging of the skin."
Melanin provides some natural defense, but research by Harvard's David Fisher and colleagues has clarified its limits — an SPF equivalent of less than 5. Crucially, their work also revealed that UV exposure is neurologically addictive, activating the same reward circuits as opiates. This helps explain why behavioural change remains so difficult even among patients who have already experienced melanoma: we are, as Fisher put it, "fighting an evolutionary drive."
The evidence base for sunscreen is substantial. A randomised controlled trial in Australia found daily use cut melanoma incidence by half, while Norwegian research linked consistent SPF 15 or higher use to a 30% reduction in melanoma risk. Studies have also shown reduced incidence of squamous cell carcinoma, basal cell carcinoma, and keratinocyte carcinomas with regular application.
Yet use remains suboptimal — partly due to misapplication, partly due to proliferating online misinformation. One critical point from Stanford dermatologists: SPF ratings are not linear. SPF 15 blocks approximately 93% of UVB radiation. SPF 30 blocks 97%. SPF 50 blocks 98%. The practical gap between SPF 30 and SPF 100 is marginal, and any broad-spectrum product applied correctly and reapplied every two hours provides meaningful protection.
| SPF Rating | UVB Blocked | UVB Transmitted |
|---|---|---|
| SPF 15 | 93% | 7% |
| SPF 30 | 97% | 3% |
| SPF 50 | 98% | 2% |
A regulatory divide has left U.S. consumers with fewer sunscreen tools than their counterparts in Europe, Asia, and Australia. Because the FDA classifies sunscreen as an over-the-counter drug rather than a cosmetic, new active ingredients face a slow, expensive approval pathway. The EU, by contrast, has approved 30 UV-filtering compounds compared to only 17 in the United States. Filters like Tinosorb, Mexoryl, and Uvinul — which offer superior long-wavelength UVA protection — remain unavailable here.
That gap is finally starting to close. In June 2026, the FDA accepted a New Drug Application for bemotrizinol — a broad-spectrum UV filter widely used in Europe and already proven safe and effective — marking the first new sunscreen ingredient accepted for U.S. review in two decades. If approved, it would be a meaningful step toward closing the protection gap that American dermatologists have long flagged.
Application tip: Stanford's Joyce Teng, MD, PhD, notes that if an active person goes through a full 6–8oz sunscreen bottle all summer, they almost certainly aren't applying enough. A bottle used outdoors regularly should last roughly two weeks with correct application.
In the mid-1990s, metastatic melanoma patients had a median survival of just 11 months, and available chemotherapies worked in roughly 15% of cases. Two decades later, immune checkpoint inhibitors and targeted therapies have fundamentally changed that calculus: half of patients with metastatic disease now survive at least five years.
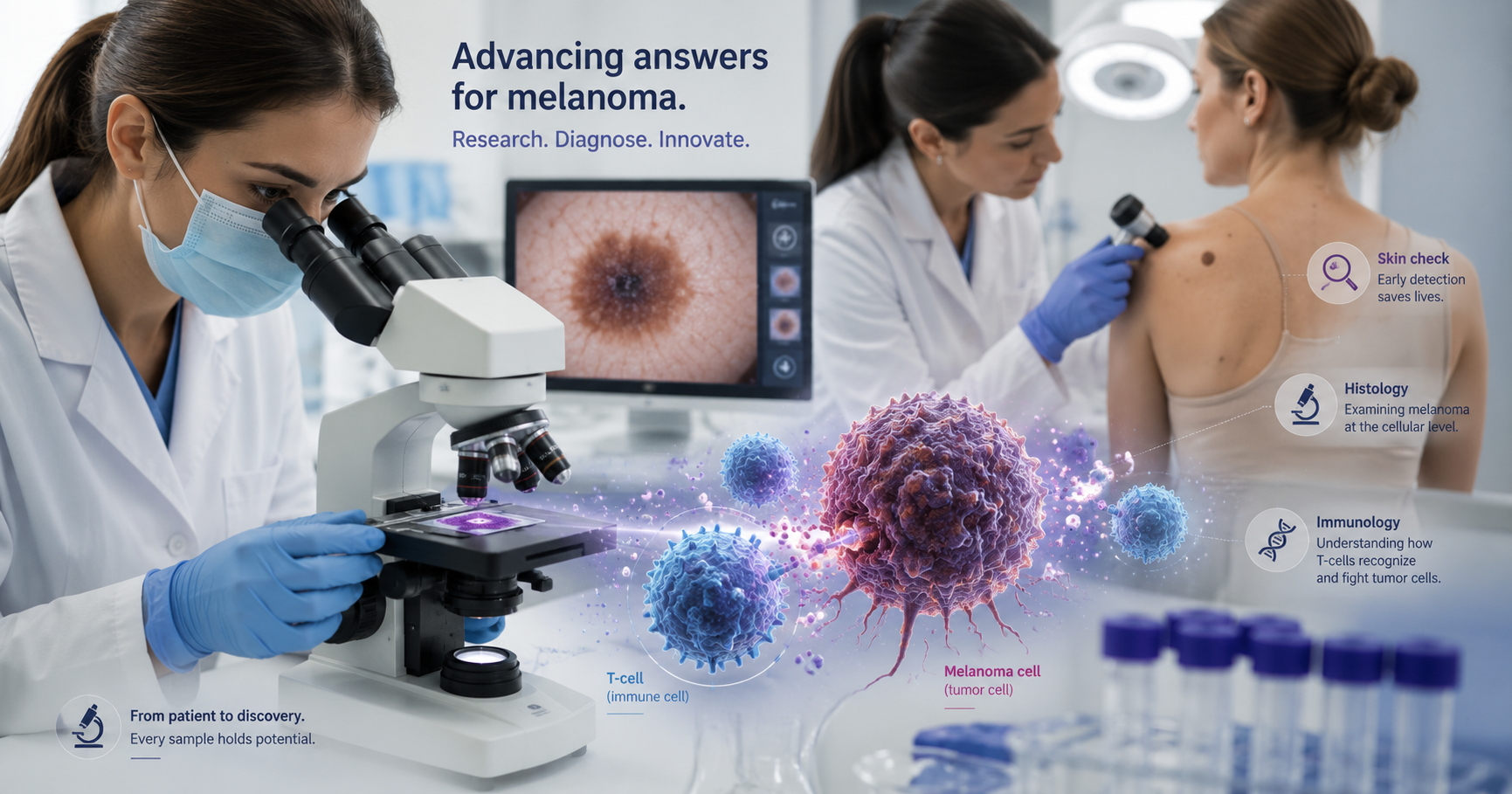
The breakthrough came from understanding how tumour cells evade immune attack. Cancer cells can express surface proteins — including PD-L1 — that bind to receptors on T cells and send a "do not attack" signal, effectively disguising themselves as healthy tissue. Immune checkpoint inhibitors, such as the CTLA-4 blocker ipilimumab (FDA-approved 2011) and subsequent PD-1 inhibitors, strip that camouflage. The approach pioneered for melanoma now treats more than a dozen other cancers.
The field is now pushing into emerging territory. Digital twin technology — creating patient-specific computational models using biologic, genomic, and environmental data — holds promise for simulating treatment responses before a prescription is written. In atopic dermatitis, the oral STAT6 degrader KT-621 has demonstrated biologics-like efficacy in moderate-to-severe disease, suggesting that the benefits of biologic precision may soon be deliverable in pill form.
Despite these advances, the field's leading researchers are quick to temper celebration. "With the advent of highly efficacious treatments, there's a tendency to celebrate the 50% who are cured," said Tsao, "and we should — but it's time to buckle down and think about the 50% who don't make it." Closing that gap requires returning to basic science alongside clinical innovation.
All statistical claims in this article draw from peer-reviewed studies, institutional research from Harvard Medical School, Stanford Medicine, and population-level data from the WHO, ACS, and NCI. Clinical expert quotes are sourced directly from published interviews and institutional publications. Specific drug efficacy claims reference FDA approval records and published trial results.
Written by
MedBary Team
Comments
Log in to join the conversation.
Loading comments…