When Your Mouth's Own Yeast Turns Against You
It looks like a food stain. It behaves like an invasion. A fungus living in 75% of healthy mouths — and it only needs one opening to take over.


A Common Infection With Uncommon Consequences
Most people dismiss a sore mouth as something they knocked with a toothbrush, but for millions worldwide, what begins as a mild irritation is the early signature of oral candidiasis — a fungal overgrowth formally documented as far back as 1838 by the French pediatrician François Veilleux. The organism responsible, Candida albicans, accounts for more than 80 percent of confirmed oral lesions and is, in the truest sense, an opportunist: it waits patiently in the mouth's microbiome until a change in the host's defences gives it room to expand.
What makes this relevant well beyond the dentist's chair is scale and reach. Oral thrush is not confined to immunocompromised patients in hospital wards. It appears in the mouths of otherwise healthy adults who have recently completed a course of broad-spectrum antibiotics. It develops in people with well-managed diabetes when blood glucose creeps upward. It surfaces in older adults wearing ill-fitting dentures, where the dampened, warm environment beneath the acrylic becomes a near-perfect incubator. And critically, it is an increasingly recognised complication for the hundreds of millions of people worldwide who rely on inhaled corticosteroids to manage asthma or chronic obstructive pulmonary disease.
Left unaddressed, oral thrush can travel. In people with compromised immunity — those receiving chemotherapy, living with HIV/AIDS, or on long-term systemic steroids — the infection can migrate down the oesophagus, a complication that turns swallowing into an ordeal and opens a pathway for systemic candidiasis. That systemic form is genuinely life-threatening and carries mortality rates in hospitalised populations that demand attention. Recognising thrush early, before it deepens, is therefore not merely a matter of comfort.
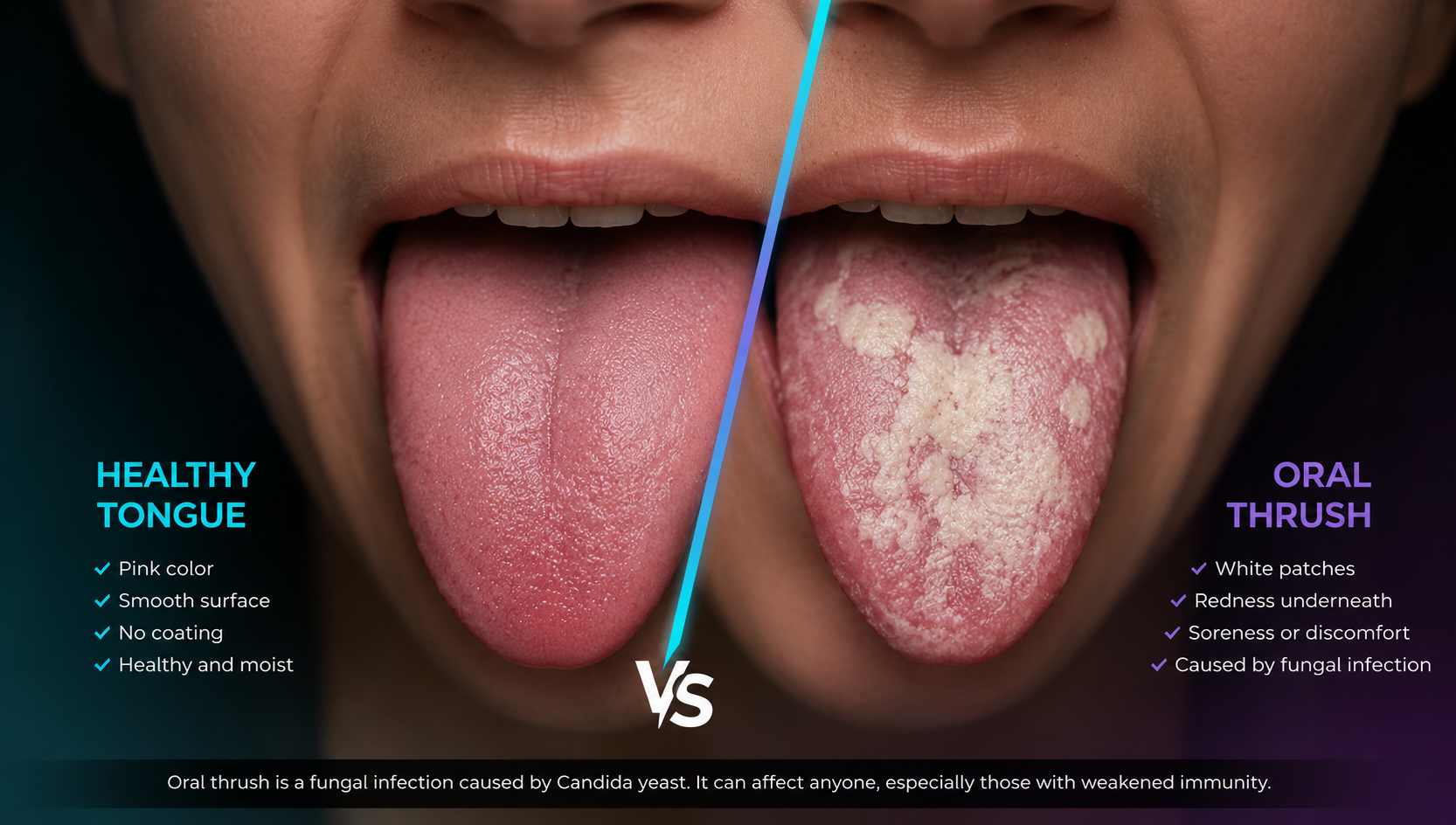
There is also the dimension of under-recognition. Oral thrush often presents without symptoms in its earliest stages — a clinical reality confirmed across multiple peer-reviewed analyses. By the time patients notice the creamy white patches, burning sensation, or altered taste that characterise the condition, the overgrowth is already established. This delayed awareness is part of why the infection persists in populations that have regular healthcare contact, and it is central to arguments for better routine oral screening.
From Root Causes to the Research Frontier
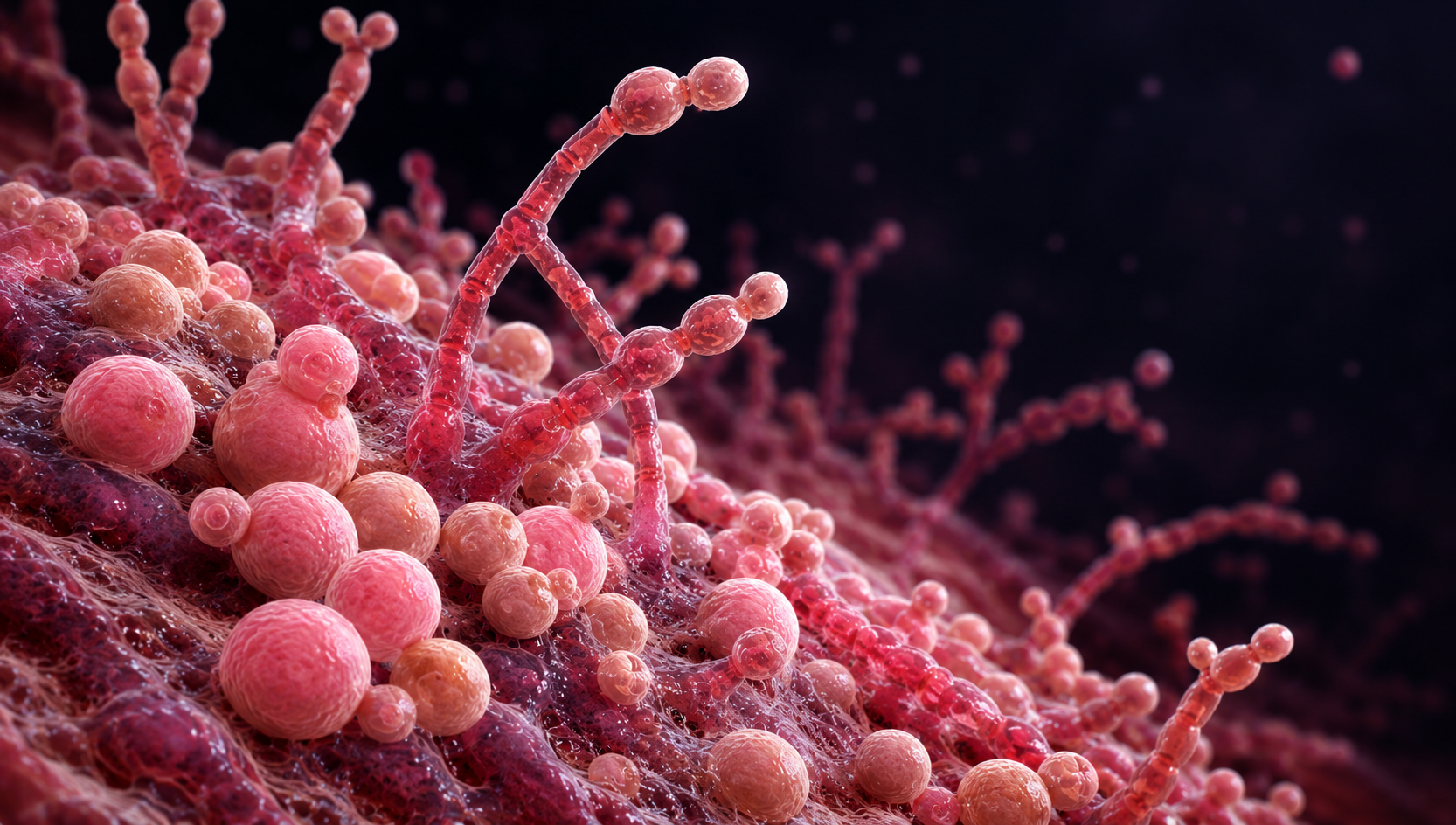
Candida albicans is a dimorphic organism — it switches between a benign yeast form and an invasive hyphal form depending on environmental cues. Under normal circumstances, the immune system, saliva's natural antifungal proteins (including histatin), and the competitive presence of oral bacteria keep it dormant and harmless. The moment any of these checks weakens, the fungus activates its filamentous, tissue-penetrating mode and begins forming biofilms — layered microbial communities that are far more resistant to antifungal drugs than planktonic yeast cells.
Antibiotic use is among the most frequent triggers. By disrupting the bacterial microbiome, broad-spectrum antibiotics remove the microbial competition that ordinarily suppresses Candida growth. Corticosteroids — whether taken orally or inhaled — suppress local immune responses. Inhaled versions specifically deposit residue in the oropharynx, creating a localised immunosuppressed environment, which explains the elevated thrush rates observed in COPD and asthma management. Poorly controlled diabetes adds another layer: elevated glucose in saliva and mucosal secretions provides a rich nutrient substrate that accelerates yeast proliferation.
The most widely recognised presentation — acute pseudomembranous candidiasis — produces the characteristic white, curd-like plaques on the tongue, inner cheeks, and palate that wipe off to leave red, sometimes bleeding tissue beneath. But clinicians describe at least half a dozen distinct presentations, including an erythematous (red) form that mimics inflammation, angular cheilitis at the mouth's corners, and a chronic hyperplastic variant whose firm white patches do not wipe away and can be mistaken for early-stage oral cancer. This diagnostic breadth means a confident lay-person assessment is often wrong, and laboratory confirmation through culture or microscopy is sometimes necessary.
Beyond visible lesions, patients frequently describe a persistent burning or soreness, a cottony sensation throughout the mouth, diminished sense of taste, and, in more advanced cases, difficulty swallowing. Infants with thrush may feed poorly, fuss persistently, or pass the infection to nursing mothers as nipple candidiasis — creating a cycle of re-infection between parent and child if only one is treated.
For most otherwise healthy adults, topical antifungal treatment resolves oral thrush without complication. Nystatin suspension — swished around the mouth and swallowed — remains the conventional first-line approach for mild-to-moderate cases. Fluconazole tablets offer a systemic alternative for patients who cannot tolerate topical preparations or whose infection is more deeply embedded. Immunocompromised patients unresponsive to first-line agents may require intravenous antifungals and specialist oversight.
Compliance is, frankly, a persistent problem. Nystatin's intensely bitter flavour prompts many patients to abandon the regimen before the infection is fully cleared — an issue that UB researcher Mira Edgerton has spent over two decades trying to solve. Her laboratory's approach uses histatin, an antifungal protein already present in human saliva, disguised with spermidine (a compound the fungus naturally absorbs) and paired with a glucosamine-based mouthwash that primes Candida to accept the compound. By exploiting the same uptake pathway the fungus uses for nutrients — a strategy borrowing from the ancient Greek concept of the Trojan horse — the treatment aims to be both more effective and far more palatable.
Separately, a 2025 investigation at Case Western Reserve University and University Hospitals Cleveland Medical Center identified a specific probiotic yeast — Saccharomyces cerevisiae — that showed measurable promise in blocking Candida albicans colonisation. The mechanism involves competitive exclusion and the disruption of biofilm architecture, offering a potential avenue for prevention rather than just treatment. This line of research is particularly significant given the growing clinical concern about antifungal drug resistance, which parallels the broader global problem of antibiotic resistance.
For inhaler users, the evidence strongly supports rinsing the mouth and gargling with water immediately after each puff — a step frequently omitted because it is not emphasised at point of prescription. Using a spacer device with metered-dose inhalers further reduces oropharyngeal drug deposition. Clinical data comparing inhaler types found that the combination fluticasone/salmeterol via pressurised metered-dose inhaler produced significantly fewer thrush cases than the dry powder inhaler equivalent — a meaningful practical distinction for prescribing clinicians.
More broadly, good oral hygiene, adequate denture care (removing and cleaning prosthetics overnight), blood glucose management in diabetic patients, and the judicious use of antibiotics all contribute to keeping the oral environment unfavourable for fungal overgrowth. These are not novel recommendations — but their consistent application remains lower than it should be across every demographic that thrush targets most.

Written by
MedBary Team
Comments
Log in to join the conversation.
Loading comments…