Why Your Blood Pressure Pills Keep Failing: The Hormone Doctors Are Only Now Learning to Test For
Your blood pressure isn't broken — your hormones might be working against your medication.

Key Highlights
More than 1 in 4 patients with treatment-resistant hypertension screened positive for excess cortisol in one of the largest U.S. studies of its kind.
Primary aldosteronism may be present in 5–10% of everyone with high blood pressure — and up to a quarter of resistant cases.
A 2025 laboratory study found estrogen raises a protective protein called ANXA1, helping shield the female heart from pressure-related damage.
Kidney “sensor” cells regulate pressure by switching a key hormone off, not only on, via calcium signals mapped for the first time in living tissue.
Women using hormonal contraceptives showed measurably higher blood pressure and BMI than non-users in a comparative clinical study.
Genetic studies now link hundreds of inherited blood-pressure gene regions directly to hormone-signaling pathways, not just lifestyle or diet.
Why It Matters
High blood pressure affects roughly half of adults in some countries, and most cases are labeled “primary,” meaning no single cause is ever pinned down. But a meaningful share of people — especially those whose numbers won't budge despite three or more medications — may be dealing with an identifiable hormonal driver rather than an unexplained condition.
That distinction matters clinically. Hypertension caused by an endocrine imbalance often responds poorly to standard first-line drugs, yet can improve dramatically once the underlying hormone problem is treated. A benign adrenal growth behind excess aldosterone can sometimes be removed surgically, effectively curing the hypertension. Excess cortisol can be managed with medication that blocks its receptor, rather than piling on more blood pressure drugs never designed to address the root cause.
It also matters because these conditions are frequently missed. Many people with primary aldosteronism have entirely normal potassium levels, so the textbook warning sign never appears. Hormone-related blood pressure changes tied to menopause, contraceptive use, or thyroid imbalance are often chalked up to aging, weight, or stress instead of being tested directly. For patients who've cycled through medication after medication without relief, a hormonal explanation can be the difference between a lifetime of trial and error and a targeted, effective plan.

Detailed Viewpoint
The Cortisol Connection
Some of the most striking recent evidence involves cortisol, the body's primary stress hormone. In a large multicenter study presented at a major cardiology meeting, more than 1,000 patients with resistant hypertension were screened using a standardized overnight test, and over a quarter met criteria for hypercortisolism — far higher than doctors had assumed. Among the subgroup with elevated blood sugar already on three or more medications, the rate climbed past 30 percent. A related trial in patients with difficult-to-control type 2 diabetes found a similar pattern, and a cortisol-blocking medication improved both blood sugar control and weight over six months. Longer-term data in patients with clinically diagnosed Cushing syndrome showed treatment could lower systolic pressure by roughly 10 points and diastolic by more than 7 points within two years, sustained out to six years. Cortisol raises blood pressure through several channels at once: it heightens blood vessels' sensitivity to constricting signals, encourages sodium retention, and interacts with the same receptor system aldosterone uses.
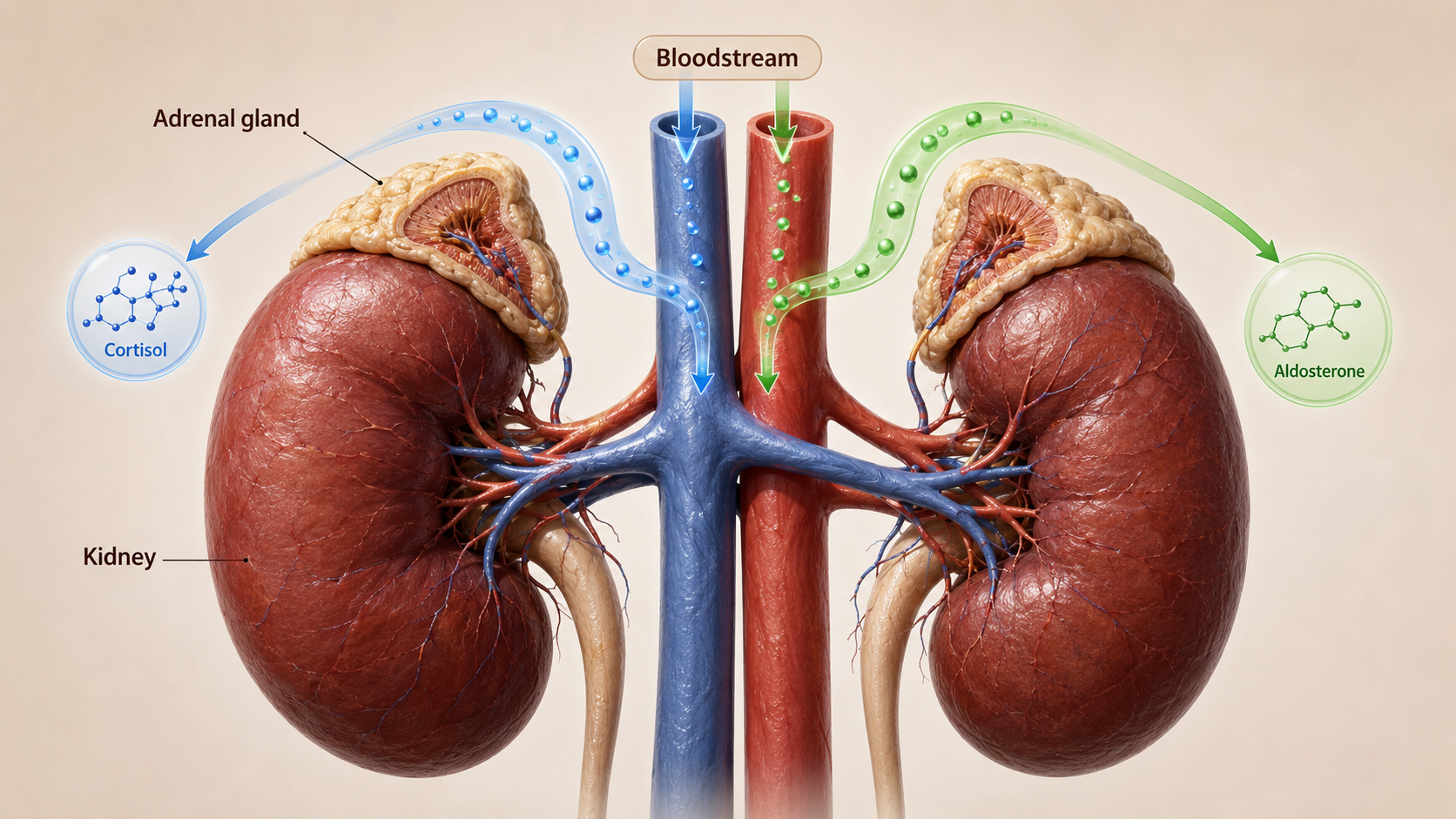
Aldosterone: The Salt-and-Water Hormone
Aldosterone, produced by the adrenal glands, governs how much sodium the kidneys hold onto and how much potassium they release. When production runs too high — primary aldosteronism — the body retains excess salt and fluid, raising blood pressure independent of diet. Researchers estimate the condition affects five to ten percent of everyone with hypertension, and as many as a quarter of those whose blood pressure resists multiple medications. Because many patients keep normal potassium levels, it's easy to overlook without a specific blood test comparing aldosterone and renin. Updated clinical guidelines now call for wider screening, particularly for anyone diagnosed before age 40, those with sleep apnea, unexplained low potassium, or a family history of the condition. Depending on the cause, treatment ranges from a minimally invasive adrenal surgery to daily medication that blocks aldosterone's receptor, often restoring control with fewer overall drugs.
The Kidney's Hormonal On-Off Switch
Newer research is also reshaping the basic science of blood pressure control. Specialized kidney cells act as the body's pressure sensors, releasing renin whenever pressure threatens to drop too low. Renin triggers a cascade that ultimately raises blood pressure, but excess renin can itself become a driver of hypertension. Scientists studying living kidney tissue recently discovered these cells rely on rhythmic bursts of calcium to shut renin production down, and that the signal spreads between neighboring cells rather than staying isolated — a far more coordinated process than earlier lab models suggested. Mapping this “off switch” could eventually lead to medications that fine-tune the renin system rather than blocking it entirely.
Estrogen, ANXA1, and the Female Heart
Sex hormones add another layer. A 2025 laboratory study found estrogen increases levels of a protective protein called annexin-A1, which helps resolve inflammation and preserve the energy-producing machinery inside heart and vessel cells. In mice lacking this protein, high blood pressure caused more severe heart and vessel damage, and the effect was more pronounced in females — one explanation for why cardiovascular disease can behave differently in women than men. The finding builds on a broader pattern: estrogen naturally relaxes blood vessels, and as levels decline after menopause, blood pressure tends to climb, while conditions marked by higher androgen levels, such as polycystic ovarian syndrome, have also been linked to elevated blood pressure risk. Researchers now hope to confirm whether the estrogen-ANXA1 relationship holds in humans, potentially supporting therapies designed specifically for women's cardiovascular health.
Contraceptives, Thyroid, and Other Overlooked Triggers
Hormonal contraceptives deserve particular attention given how widely they're used. A comparative study of 290 women found that those using oral pills, injectables, or implants had significantly higher blood pressure and body mass index than non-users, even though their blood electrolyte levels stayed essentially the same. The likely mechanism involves estrogen's stimulating effect on a liver protein that feeds into the same renin-driven pathway implicated in kidney-based hypertension — a reminder that routine blood pressure monitoring matters for anyone starting or continuing hormonal birth control. Thyroid imbalances add another pathway: an underactive thyroid tends to raise the lower (diastolic) number, while an overactive thyroid tends to raise the upper (systolic) number, alongside symptoms like fatigue, weight changes, or a racing heartbeat. Rarer causes, including adrenal tumors that release adrenaline-like hormones or glands that overproduce parathyroid hormone, round out a growing list of endocrine conditions specialists now test for in the right circumstances.
Is High Blood Pressure Really “Hereditary”?
Family history remains one of the most common explanations patients hear for their hypertension, and it's often accurate — but the story runs deeper than a single inherited trait. Large genetic studies have identified hundreds of gene regions that each nudge blood pressure slightly, many tied directly to the same hormone pathways described above, including the renin-angiotensin-aldosterone system. That means an inherited tendency toward high blood pressure may, in many people, really be an inherited tendency toward a specific hormonal imbalance — one that, unlike a static genetic label, can potentially be identified and treated.

Citation & Credibility
This article draws on peer-reviewed research and reporting from Harvard Health Publishing, the University of Virginia School of Medicine, Monash University, the Singapore Heart Foundation, the Endocrine Society and its regional affiliate bodies, Karolinska Institutet, and a peer-reviewed comparative study published in the Ethiopian Journal of Reproductive Health, alongside findings presented at major cardiology and endocrine conferences. Clinical figures and study findings are sourced from institutional news releases, journal publications, and conference proceedings current as of 2026.
This content is intended for general educational purposes and does not replace individualized medical advice. Anyone concerned about resistant or unexplained high blood pressure should speak with a physician or endocrinologist about appropriate hormonal screening.
Written by
MedBary Team
Comments
Log in to join the conversation.
Loading comments…