
Remote Care Expands Access for Sickle Cell Disease Patients, but Adult-Caregiver Disparities Persist
Remote video and phone consultations have opened a critical doorway for sickle cell disease (SCD) patients, with overall satisfaction reaching over 90% among both adults living with the condition and caregivers of affected children — yet a widening gap in experience and home support between these two groups reveals that virtual care is not yet reaching its full potential for adult patients.

A 2024 cross-sectional study led by researchers within the Pacific Sickle Cell Regional Collaborative found that caregivers consistently reported higher satisfaction, greater home support, and stronger access to remote care infrastructure than adults managing SCD independently — raising urgent questions about equity, digital literacy, and the adequacy of specialist care for one of America's most underserved chronic disease populations [1].

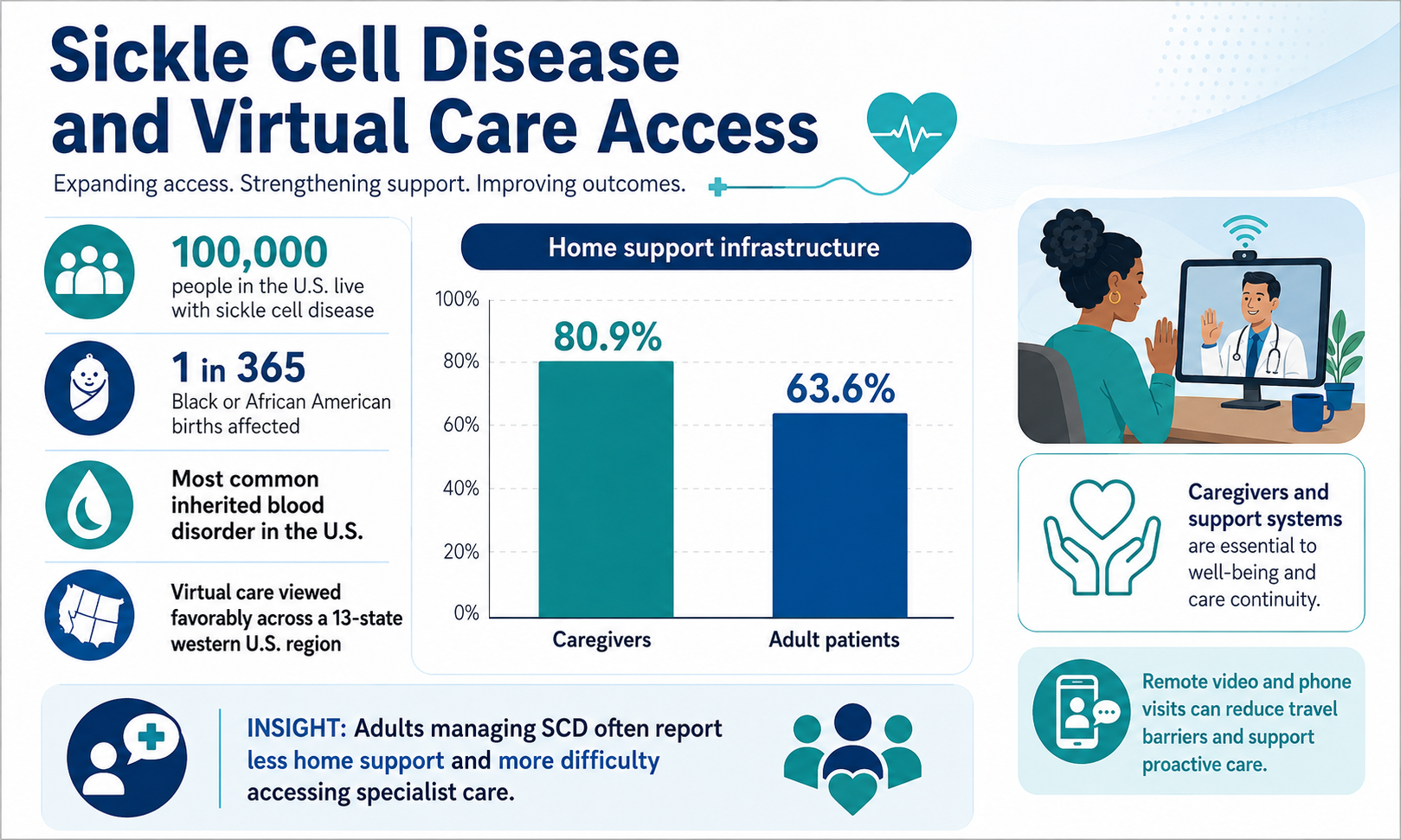
An estimated 100,000 people in the United States live with sickle cell disease — with roughly 1 in every 365 Black or African American births affected — making it the country's most common inherited blood disorder [2][3]. The disease causes abnormal, sickle-shaped red blood cells that block blood flow, triggering severe pain episodes, progressive organ damage, stroke, and in many cases premature death. Despite this immense burden, access to trained SCD specialists has remained persistently scarce, particularly for adults who have transitioned out of paediatric care [1].
Remote video and phone-based consultations gained rapid traction during the COVID-19 pandemic as a practical workaround to the specialist shortage, and the evidence gathered since suggests genuine promise. The PSCRC study found that most participants across a vast 13-state western US region viewed virtual care favourably [1]. For patients in rural or geographically isolated settings where in-person SCD specialists simply do not exist, even imperfect remote access can mean the difference between proactive managed care and recurring, crisis-driven emergency room visits — a pattern that carries enormous personal cost and a broader systemic burden on healthcare resources [6].
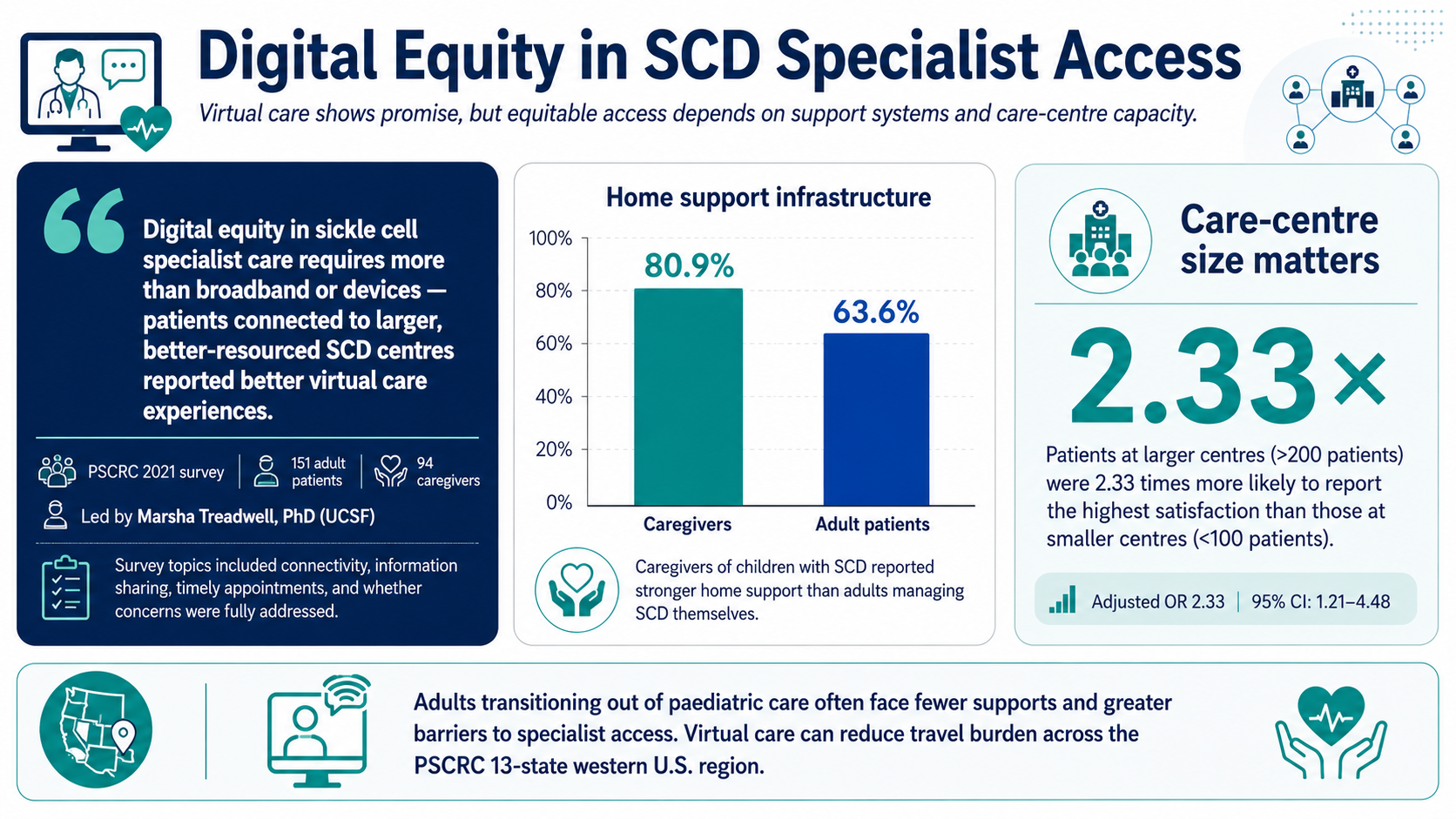
Yet the satisfaction gap between caregivers and adult patients is far more than a statistical footnote. Caregivers of children with SCD reported markedly better home support infrastructure (80.9% versus 63.6% for adults) and were substantially more likely to give the highest rating [1]. Adults managing SCD themselves — often socioeconomically disadvantaged, frequently on public insurance, and navigating the condition without the scaffolding of paediatric care — are the very people most in need of equitable specialist access. The data suggest they are not yet reliably receiving it.
The research, led by Marsha Treadwell, PhD, a professor in the Department of Pediatrics at the University of California San Francisco, drew on surveys completed in 2021 by 151 adult patients and 94 caregivers within the Pacific Sickle Cell Regional Collaborative (PSCRC) — one of five HRSA-funded regional programs established to strengthen SCD care access across the United States [1]. The 30-item online survey assessed both technical dimensions (reliable internet connectivity, ease of health information sharing) and experiential ones (whether appointments started on time, whether patients felt their concerns were fully addressed). The design captured what remote specialist care actually feels like in practice, not just whether it technically functions.
One of the study's most consequential findings concerned care centre size and its relationship to satisfaction. Patients seen at larger centres — treating more than 200 patients — were 2.33 times more likely to report the highest level of satisfaction compared to those at smaller centres treating fewer than 100 patients (adjusted OR: 2.33; 95% CI: 1.21–4.48) [1]. Larger centres typically have dedicated administrative infrastructure, greater experience with remote care delivery, and better-resourced clinical teams — advantages that produce smoother, more consistent specialist encounters. This finding carries significant policy weight: improving equitable access requires investing in the organisational capacity of SCD care centres, not simply expanding broadband access or distributing devices [1][6].
The role of navigation assistance offered an important and nuanced signal. Counter-intuitively, participants who required help from a navigator were actually less likely to award the highest satisfaction rating (adjusted OR: 0.37; 95% CI: 0.19–0.71) [1]. The researchers interpreted this not as evidence that navigation harms the experience, but as a sign that those requiring help were patients already facing greater underlying barriers — technology access difficulties, lower digital confidence, or more complex socioeconomic circumstances. Navigator support is valuable, but it cannot fully compensate for deeper structural disadvantages in a single clinical interaction. Closing the gap will require upstream interventions: digital literacy programming, dedicated hardware access, and community health worker support integrated directly into SCD care models.
The broader clinical context deepens the urgency. The American Society of Hematology has long emphasised that SCD care is disproportionately managed through emergency departments rather than in continuous, specialist-led relationships — a pattern driven by provider shortages, implicit bias in pain management, and fragmented insurance coverage [3][4]. Patients with SCD are hospitalised more frequently than those with other chronic diseases of similar severity, and care facilities treating fewer SCD patients tend to produce worse outcomes, reflecting an experience and skills gap among providers [6]. Remote specialist consultations, when functioning well, offer a pathway to more consistent oversight that reduces emergency dependence. When they function unevenly — as the PSCRC data suggest they do for adult patients — the risk is that digital inequality replicates the same disparities that have long characterised in-person SCD care.
Looking ahead, the study's authors explicitly called for continued vigilance about differences in digital literacy and technology access as potential drivers of widening care disparities [1]. As remote consultation transitions from a pandemic-era emergency measure into a permanent feature of SCD care delivery, health systems, payers, and patient advocacy organisations must ensure that adults with SCD — who are predominantly Black or African American, frequently socioeconomically disadvantaged, and historically undertreated for pain [5] — are not left behind in a care model that currently works far better for the families of affected children than for patients managing the disease themselves [1].
- [1] Treadwell M, Du L, Lawrence Y, Gaspar M, Hassell K, Shah S, Akpan M, Crook N, Taylor M, Gopal S; Pacific Sickle Cell Regional Collaborative — "Tracking Remote Care Needs for Individuals With Sickle Cell Disease Through the COVID-19 Pandemic: A Cross-Sectional Survey Study", Health Science Reports, November 5, 2024. Source: doi:10.1002/hsr2.70163
- [2] Centers for Disease Control and Prevention — "Data & Statistics on Sickle Cell Disease", CDC.gov. Source: https://www.cdc.gov/sickle-cell/data/index.html
- [3] American Society of Hematology — "Sickle Cell Disease: Patient Information", Hematology.org, 2024. Source: https://www.hematology.org/education/patients/anemia/sickle-cell-disease
- [4] American Society of Hematology — "ASH Position Statement on Sickle Cell Trait", Hematology.org, 2021. Source: https://www.hematology.org/advocacy/policy-statements/2021/ash-position-on-sickle-cell-trait
- [5] Sick Cells — "2024 Medicaid Access and Landscape Review for Sickle Cell Disease", SickCells.org, 2024. Source: https://sickcells.org/research/2024-medicaid-access-and-landscape-review-for-sickle-cell-disease
- [6] Lee L, Smith-Whitley K, Banks S, Puckrein G — "Reducing Health Care Disparities in Sickle Cell Disease: A Review", Public Health Reports, 2019. Source: doi:10.1177/0033354919881438
Editorial Note: This article is produced for informational and educational purposes. It does not constitute medical advice. Patients should consult a qualified healthcare provider for diagnosis and treatment guidance. All statistics cited are sourced from peer-reviewed literature or named patient advocacy organizations as referenced above.
Written by
MedBary Team
Comments
Log in to join the conversation.
Loading comments…